Query
What concrete steps can donors and countries receiving vaccines take to mitigate risks of diversion and corruption related to the COVAX COVID-19 vaccine rollout?
Background
Tackling corruption is crucial for inclusive human and economic development; during crises it becomes indispensable to ensure an effective response and a sustainable recovery, a point brought into sharp focus by the ongoing Covid-19 pandemic (Kohler et al. 2016; Thorp 2020; UN News 2020; Jenkins et al. 2020; Duri 2021).
The United Nations Secretary-General, António Guterres, has warned that “corruption drains resources from people who need them, undermines trust in institutions, exacerbates the vast inequalities exposed by the virus, and hinders a strong recovery”, adding that recovery from Covid-19 “must include measures to prevent and combat corruption and bribery” (UN News 2020).
Corruption has been shown to have particularly pernicious effects on the health and pharmaceutical sector and is anathema to Sustainable Development Goal 3, which aims to “ensure healthy lives and promote well-being for all at all ages” (Bruckner 2019).
Given the scale and complexity of manufacturing, allocating and distributing Covid-19 vaccines around the world, there is growing concern that rampant corruption could undermine the effectiveness of the global inoculation campaign (UNODC 2020).
One of the key mechanisms being used by governments to acquire vaccines is Covid-19 Vaccines Global Access (COVAX), which is jointly run by the Coalition for Epidemic Preparedness Innovations (CEPI), Gavi the Vaccine Alliance, the World Health Organisation (WHO) and the United Nations International Children’s Emergency Fund (UNICEF) (WHO 2021).
Ninety-two low- and middle-income countries will be able to access vaccines through the COVAX Advance Market Commitment (AMC) at the same time as high-income countries. The list of COVAX AMC donor commitments is found here. The aim of the mechanism is to protect at least 20% of each participating country’s population by the end of 2021. COVAX AMC enables AMC-eligible economies to receive fully subsidised donor-funded doses (COVAX 2020; Berkley 2021).
Figure 1: Showcasing the sequenced vaccine rollout stages and target groups. Source: BBC News 2021.
Yet as of March 2021, only 14% of the world’s Covid-19 vaccines had been purchased by COVAX (Transparency International 2021). Samantha Power, the Biden administration’s nominee to be administrator of the United States Agency for International Development (USAID) – the largest single donor to COVAX – has argued that its vaccination goal is “not sufficient” and would need to be “supplemented by bilateral donations, [and] surplus donations” (Oswald 2021).
Currently, high-income countries have procured more than half the supply of Covid-19 vaccines, while low-income countries have been largely left behind (The New Humanitarian 2021; Transparency International 2021). Many wealthier governments are bypassing the COVAX mechanism to strike bilateral deals with Covid-19 vaccine manufacturers. This behaviour has further raised equity concerns about restricting the supply of vaccines to low- and middle-income countries, as well as the inflationary effect on prices (Transparency International 2021). For example, South Africa is set to buy doses of Oxford-AstraZeneca’s vaccine at a price nearly 2.5 times higher than most European countries (Sullivan 2021).
The nature of the challenge at hand and the fact that demand for vaccines far outstrips supply has resulted in a fierce competition between countries, the proliferation of confidentiality clauses between governments and pharmaceutical companies, and consequently widespread opacity in the acquisition of vaccines (Baker 2020; Upton 2020; Transparency International 2021). In this context, reports of substandard and falsified vaccines found across several countries are deeply alarming (Interpol 2021; Reuters 2021).
Covid-19 has created the perfect storm for corruption by producing new opportunities for rent-seeking. More domestic and foreign resources have been made available to contain the pandemic in a context where there is further discretion in decision-making and the allocation of resources combined with limited supervision and enforcement. (Martini 2020).
Mapping corruption vulnerabilities in Covid-19 vaccine rollout requires an understanding of the pharmaceutical value chain. Such an analysis offers a framework to examine the scale and impact of corruption issues affecting vaccines from the laboratory through to its distribution to a healthcare facility, and subsequent administration to the patient (Kohler et al. 2016). There are several actors involved as well as different corruption risks at each level of the vaccine value chain. These are summarised in the table below (from Kohler et al. 2016 and UNODC 2020).
Table 1: Stakeholders and corruption risks across the vaccine value chain
|
Stage of Vaccine Value Chain |
Main actors at each stage |
Potential corruption risks |
|
Research and development |
Pharmaceutical companies |
Perverse incentives; regulatory capture; conflict of interest |
|
Clinical trials and approvals |
Pharmaceutical companies; medical agencies; regulatory authorities |
Conflict of interest; bribery; ghostwriting[1] |
|
Manufacturing |
Pharmaceutical companies; organised criminal groups |
Substandard, spurious, falsely labelled, falsified and counterfeit (SSFFC) medicines/vaccines; bribery by manufacturers for the certification of Good Manufacturing Practices (GMP) or deliberate lack of adherence to GMPs when certificates have been awarded to increase profits; creation of entry barriers for competitors
|
|
Registration |
Pharmaceutical companies; regulatory agencies |
Bribery and other forms of corruption to seek shortcuts to register medical products; use of inappropriate registration procedures if they lack sufficient oversight |
|
Marketing |
Pharmaceutical companies |
Medical ghostwriting; falsified information; bribes |
|
Procurement |
Procurement agencies; brokers; middlemen |
Collusion; kickbacks; clientelism; false invoicing |
|
Delivery |
Distributors; public authorities, e.g. customs officials |
Theft; conflict of interest; substandard and falsified medicines can also infiltrate health systems during the delivery stage. |
|
Targeting |
Public authorities |
Mismanagement; patronage; favouritism |
|
Distribution |
Healthcare providers; brokers; middlemen |
Theft; bribery; patronage; favouritism; conflicts of interests; undue influence |
[1] Ghostwriters in medicine are medical writers that publish favourable articles in medical journals, which can influence doctors and policymakers in decisions that affect healthcare (Langdon-Neuner 2008).
This Helpdesk Answer will focus on corruption risks in the latter stages of this value chain, given that, as of March 2021, the most pressing concern is to minimise corruption in the delivery, targeting and distribution of Covid-19 vaccines.
It is important to note that, depending on the country’s context, there may be a range of actors involved in the acquisition, storage, transportation and distribution of vaccines, as well as influencing the targeting policy and prioritisation of risk groups. These actors can be both licit and illicit.
While public officials and politicians are almost invariably involved, others can play significant – and potentially contentious – roles. In Uganda, for instance, the inter-agency Covid-19 taskforce is led by the army in a bid to support the health ministry. While the military has played a role in supporting treatment of Covid-19 patients, accountability gaps and use of excessive force are seen as common features of the military in the country and could undermine the integrity of the process and people’s human rights (Namwase 2020). In a similar vein, national armies in Myanmar, Indonesia and Thailand have reportedly marginalised civilian authorities and taken frontline control over the Covid-19 response (Graham 2020).
Middlemen and brokers may also play a substantial role in vaccine distribution. While not related directly to the vaccines, a number of high-profile scandals involving German politicians taking large commissions to act as middlemen between manufacturers and consumers have illustrated the heightened risk of collusion and kickbacks that such arrangements could entail for the vaccine rollout (Chazan 2021).
This is particularly worrying given the widespread trend of governments easing due diligence processes and oversight mechanisms to procure goods and services urgently needed to tackle the pandemic (Beuter 2020; OECD 2020; O’Dowd 2021).
Those seeking to reduce the risk of corruption in vaccine rollout would do well to be mindful of broader contextual factors that could shape the nature of corrupt behaviour in different settings. This could include, for instance, the role of the private sector. For instance, Pakistan is one of the first countries to allow the private sector to import and sell Covid-19 vaccines. While the global price for the Russian vaccine Sputnik V is estimated to be set at US$20, each dose is currently being sold at rates inflated by over 150% in Pakistan (Osborn and Nikolskaya 2020; TI Pakistan 2021). Such market conditions create lucrative opportunities for unscrupulous actors.
Other relevant structural factors include the state of a country’s health information management system.9e9cd6e5ee4f Apart from being essential for monitoring and evaluation, health information systems also provide an alert and early warning capability, supporting patient and health facility management, enabling planning, supporting and stimulating research, permitting health situation and trends analysis, supporting global reporting and underpinning communication of health challenges to diverse users (WHO 2008). Thus, such information systems would be key to identify and prioritise risk groups and deliver the required number of vaccines when and where they are needed. One example is District Health Information Software 2 (DHIS2),b1135dd8403f which has developed toolkits to support Covid-19 surveillance and national vaccine delivery plans usable throughout Asia, Africa and Latin America (DHIS2 2021b).
In countries with poor quality health data, or where a large number of citizens lack formal identity documents, it will be much easier for corruption to go undetected. This could include the supposed delivery of the vaccine to “ghost beneficiaries”, while corrupt actors pocket the vaccines or public resources intended to benefit citizens. The Philippines’ management of Covid relief funds is a case in point: around 3% of those receiving these funds were ghost beneficiaries. While not related to vaccine rollout, this example highlights the risks stemming from contexts with low levels of public health data (GTAI 2020).
Another consideration is the type of vaccine in question. Different vaccine cold chainse791ca61f6c4 will require different storage and transportation needs, which could affect the kind of actors and corruption risks involved.
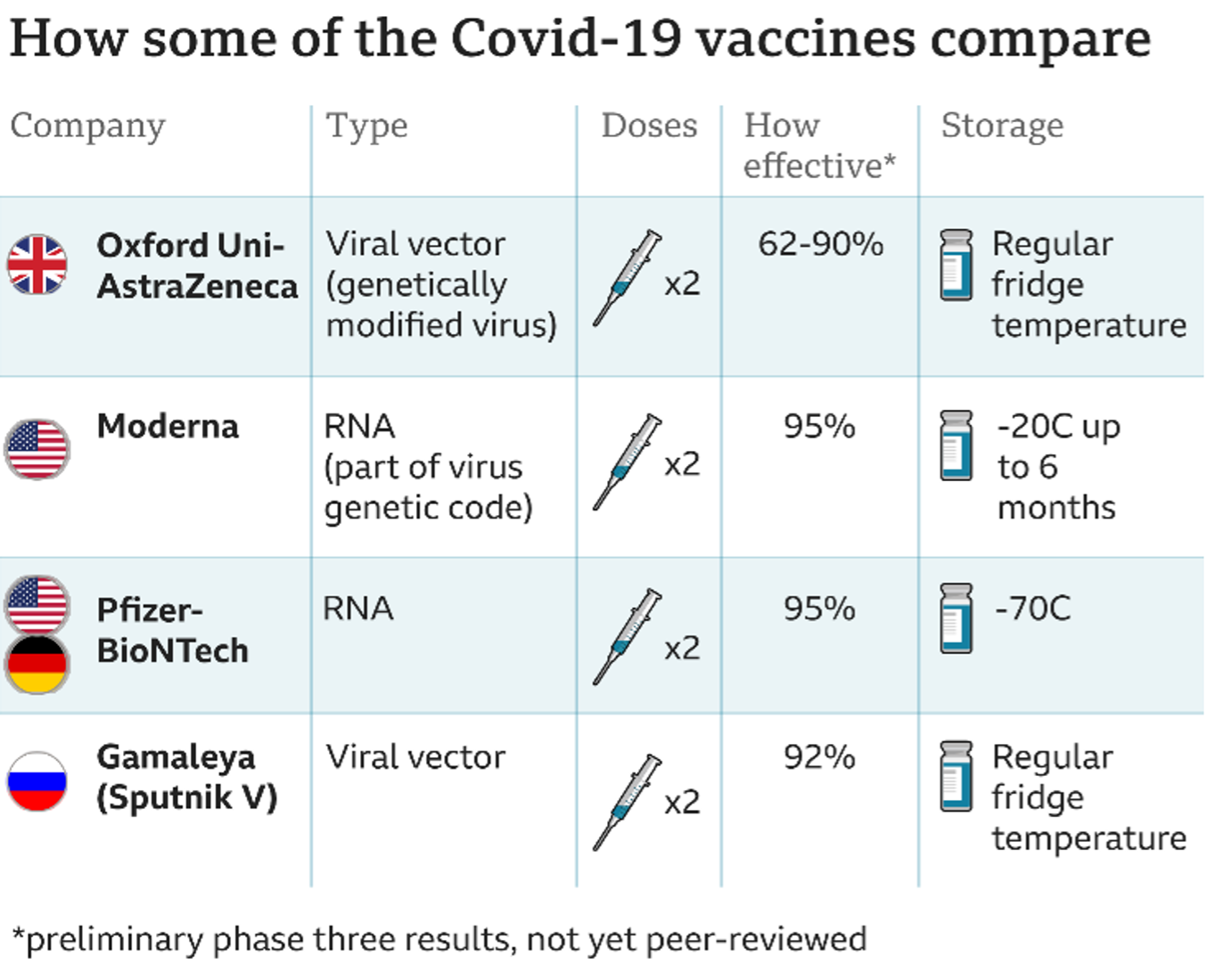
Figure 2: Comparison of COVID-19 vaccines. Source: Mwai 2021.
The Pfizer-BioNTech vaccine, for example, was not considered suitable for mass vaccination in South Africa due to its storage requirements of -70C, which would pose technical challenges and involve another layer of stakeholders in the distribution process (Mwai 2021).
More generally, as illustrated in figure 3, the numerous interactions involved in delivering vaccines to citizens – from manufacturers to logistics firms, from procurement agencies to couriers and onto health workers – provide a wide range of entry points for the corruption risks listed in Table 1.
Before an overview of the corruption risks involved in the delivery, targeting and distribution of vaccines, it is worth noting that focusing on vaccines should not come at the expense of tackling corruption affecting the procurement and distribution of other key medical supplies. These include personal protective equipment and ancillary goods such as syringes.
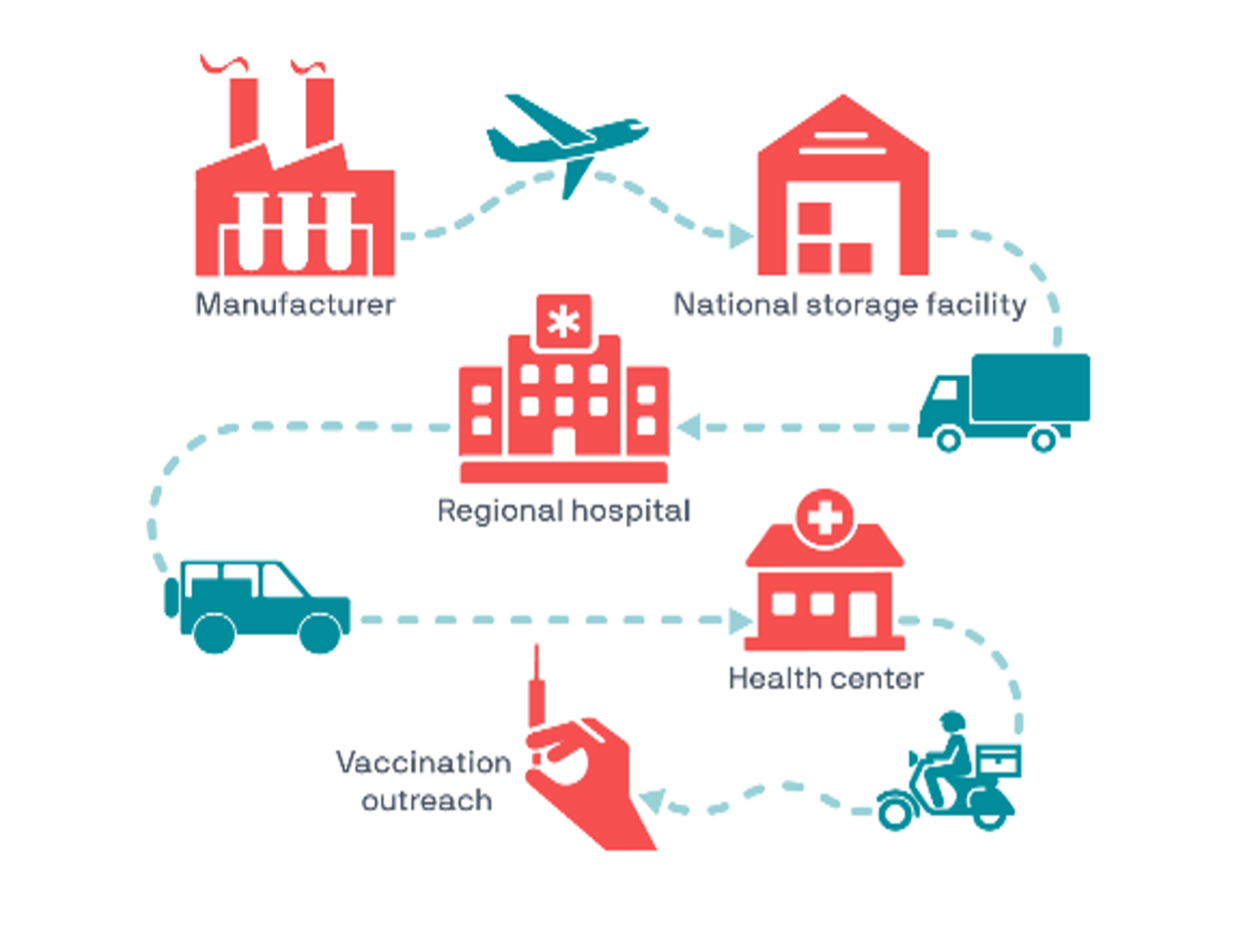
Figure 3: Illustrative vaccine cold chain. Source: Path 2021.
Corruption risks
Vaccine deployment is subject to corruption risks throughout the entire process. UNODC (2020) lists the following as the main corruption risks in Covid-19 distribution:
- theft of vaccines within the distribution systems, which can lead to the proliferation of substandard and falsified medicines in black markets
- leakages in emergency funding designated for the development and distribution of vaccines
- nepotism and favouritism
- corrupted procurement systems
- conflict of interest
- undue influence of companies
The ongoing pandemic has already shown that items in high demand and short supply, such as personal protective equipment (PPE), swabs, ventilators and potential therapeutic medicines, are especially vulnerable to fraud and corruption (Thorp 2020).
Women and girls are particularly vulnerable to corruption across the healthcare system, both as patients and providers, and through sextortiona909714213d2 (Transparency International 2020). Experiences of sextortion in vaccine and aid distribution have been documented in the past. For example, during the Ebola epidemic,in the Democratic Republic of the Congo (DRC), allegations that women were being asked for sexual favours in exchange for treatment were levelled against the vaccination programme being run in the country (Holt and Ratcliffe 2019).
The next section briefly considers corruption risks in the delivery, targeting and distribution stages of the vaccine value chain and provides some documented examples from the current pandemic.e4017106523e The paper looks at contextual, organisational, individual and working process factors to identify the highest corruption risks.
Contextual factors
These relate to background factors outside of the control of those charged with acquiring and distributing vaccines, as well as identifying priority groups for inoculation.
Specific risk factors
- lack of, unclear or inconsistent basic legal framework needed to counter corruption and strengthen integrity (such as effective criminal and civil codes, conflict of interest laws, free access to public information laws, asset disclosure rules, codes of conduct, lobbying regulation and whistleblower protection)
- unclear competences of the authorities responsible for vaccine rollout
- unadjusted or disharmonised work of public sector institutions, which can lead to duplication and/or waste of resources
- inefficient law enforcement and prosecution
- inefficient or incompetent oversight institutions or supervisory authorities
- non-transparent public finance processes
Vaccine hesitancy is a significant contextual factor related to trust (Butler n.d.; Kiley 2016). The refusal to accept available vaccines is a critical barrier to achieving a comprehensive, global distribution (Trogen et al. 2020). Long-standing corruption has contributed to a general lack of public confidence in many governments. This, together with expedited approval processes and misinformation around vaccines are contributing to vaccine hesitancy (Kiley 2016; Meeme 2020).
Examples
Rwanda’s COVID-19 vaccination rollout is reportedly characterised by secrecy, and there is some confusion around the type of vaccine being used as well as the source of its procurement (Nakkazi 2021).
In Iran, the unclear division of power between the government, and the Supreme Leader is viewed as having hampered the institutional response to COVID-19 (Darian 2021).
A constitutional crisis in Haiti that has prompted unrest and bureaucratic chaos is overshadowing the country’s COVID-19 vaccine rollout. The ensuing distrust of government is reportedly fanning scepticism towards vaccines among the population (Obert 2021). Similarly, in Ukraine, according to a recent poll by the Kyiv Institute of Sociology, 60% of the respondents did not want to be vaccinated against COVID-19. According to Mamo (2021), distrust of the government is the key factor.
In Moldova, the president acknowledged that the country’s weak institutions and their susceptibility to corruption are hampering vaccine rollout (Euronews 2021).
The EU position on transparency when negotiating advance purchase agreements (APAs) is that, while it recognises its importance, “due to the highly competitive nature of this global market, the commission is legally not able to disclose the information contained in the contracts” (Sciacchitano and Bartolazzi 2021).
Pfizer has informed its investors that as early as next year they are going to be moving away from “pandemic pricing” towards price points that are on par with other vaccines that they have on the market, at US$150 or $175 per dose (Belli 2021).
Organisational factors
These include factors within the control of the entities involved in the vaccine rollout that are the result of their actions or inactions, such as the rules and policies, management, decision-making, operational guidance and other internal regulations.
Specific risk factors
- poor strategic and operational guidelines or inadequate policies, procedures or systems
- chronic failure to follow existing policies, procedures or systems
- unclear mandate of an institution, project, etc.
- poor or inconsistent internal acts and regulations
- absence of warning and alert systems in case of different types of irregularities
- weak managerial and administrative measures against corruption
- inadequate/weak work review, supervision, oversight or control procedures and audit mechanisms
- absence of rules and procedures that promote ethical behaviour and transparency
- inadequate or insufficient systems for training and educating public officials, including superiors and supervisors
- inadequate human, finance or time resources in the organisation or its teams high levels of power or influence, not consistent with their actual position
Examples
A memorandum of understanding between AstraZeneca and a Brazilian manufacturer, defines the “Pandemic Period” as ending on 1 July 2021. The period could be extended on condition that “AstraZeneca acting in good faith considers that the SARS-COV-2 pandemic is not over”. Such clauses allow manufacturers plenty of room to increase the costs of their vaccine (Financial Times 2021).
On the issue of ghost beneficiaries, in Colombia, several ID numbers from deceased people have been prioritised for vaccination in the online platform Mi Vacuna, raising fears of corruption infiltrating the government’s selection of priority groups and distribution of Covid-19 vaccines (Semana 2021).
Observers in Malawi have voiced concern that determining priority groups at the local level is being done in a non-scientific way. For instance, when it comes to targeting beneficiaries, authorities are estimating that about 5% of the population in each village is elderly (Republic of Malawi 2021). Such numbers may be unlikely given the national demographics (UNPD 2019) and leave the door open to manipulation and abuse by unscrupulous actors.
Opacity shrouding emergency procurement processes has resulted in contracts being kept of the public eye. For instance, public disclosure of Hungary’s contracts for purchase of Sinopharm and Sputnik V vaccines reveals that the country has paid a higher price than other countries for Sinopharm. The Sputnik contract on the other hand places the liability of all adverse events, side effects, problems due to insufficient efficacy, poisoning and allergic reactions or any other negative event, onto the customer (Tanács 2021).
Individual factors
These are factors that could motivate individuals to engage in corrupt or unethical behaviour.
Specific risk factors
- lack of knowledge or integrity
- pressures in the operating environment
- prevailing social norms that incentivise corruption
- inadequate supervision or performance review
- inappropriate relationship with clients
- omission of conflict of interest declarations
- feelings of dissatisfaction or perceptions of unfairness
Examples
Theft of vaccines within the distribution systems are not limited to developing contexts. In the United States, theft and inappropriate administration of vaccines has been documented already (Silverman et al. 2021; Vigdor 2021).
In the United Kingdom, several vaccination centres state that many people are falsely claiming they are frontline health or social care workers when they book an appointment. Pharmacists delivering vaccine doses are having to police the process to ensure that target beneficiaries receive the vaccine (Lynn 2021).
Transparency International Bangladesh (TI-B) has highlighted the problem of political actors and activists being involved in widespread corruption of various types, including embezzlement, hoarding and misappropriation of relief goods intended for the Covid-19 response (TI Global Health Programme).
Working process factors
These include factors that arise from working procedures in an organisation.
Specific risk factors:
- high levels of personal discretion
- non-transparent or unrecorded decision-making
- poor organisation of operating processes
- lack of participation of multiple stakeholders, including women and representatives of other marginalised groups affected by the pandemic
- unconnected work process and procedural gaps
- lack of vertical and horizontal controls in the operational processd01bd42b9e45
Examples
Nepotism/favouritism: line-cutting behaviour of high-level political leaders and wealthy individuals trying to access the vaccine ahead of their turn has been witnessed in Kenya, Canada, Peru, Argentina, Spain, Brazil and Poland (Al Jazeera 2021; BBC News 2021b; DW 2021; Taj et al. 2021)
Proliferation of black markets for substandard and falsified Covid-19 vaccines have been encountered in Mexico, the Philippines and Nigeria, among other countries in Latin America, Africa, and Asia (Cabato 2021; NAFDAC 2021; Valadez 2021).
Mitigation measures
The following section considers broad areas in which donors could act to reduce risks of corruption in the Covid-19 vaccine rollout. Where possible, these seek to build on existing processes and platforms.
Donor support to transparency measures and access to information
Strong transparency provisions are crucial to vaccination efforts for two reasons. First, research compiled by the Pandemic Action Network (2020) has found that government transparency with regards to vaccination schemes is an important means of increasing citizen trust in the efficacy and safety of vaccines. Second, embedding transparency into planning, administration, monitoring and appraisal of distribution, targeting and delivery mechanisms is essential to minimise the risk that corruption hinders vaccination programmes (TI Global Health Programme 2021).
Transparent targeting
When it comes to identifying risk groups and prioritising the allocation of vaccines, there is a risk that undue influence and political bias will skew precious resources away from those most in need.
In most countries, National Immunisation Technical Advisory Groups (NITAGs)04956614fbbb play a key role in identifying target populations. However, in many settings there is a lack of relevant national data and evidence on key populations, which makes it difficult for NITAGs to develop evidence-based distribution strategies in line with the WHO SAGE framework recommendations for the allocation and prioritisation of COVID-19 vaccination (WHO 2020; TI Global Health Programme 2021).
The lack of reliable or available data on target populations has a direct impact on healthcare service delivery (TI Global Health Programme 2021). For instance, reports on access to healthcare in Zambia, Uganda and Bangladesh from Transparency International Health Initiative highlight that bias, undue influence and poor planning results in the exclusion of people from socio-economically deprived backgrounds, and disproportionately affect women (TI Global Health Programme 2021).
To counteract nepotism, favouritism, undue influence and political bias in identifying target groups, planning for vaccine distribution and the identification of vulnerable populations needs to be transparent. This is to ensure that access is equitable, and citizens are in a position to understand who will receive vaccines and who will not (Cushing 2021; TI Global Health Programme 2021).
Donors could support aid-recipient countries by providing technical assistance to NITAGs to develop transparent targeting criteria that set out clear guidance on prioritisation. When defining target groups, it is key to avoid ambiguities or loopholes that create the potential for abuse.
Participatory consultation with marginalised and at-risk groups can help ensure their needs are reflected in the distribution strategy. Donors could also support NITAGs to use and, where possible, refine national health information management systems as a means of identifying vulnerable populations. As mentioned earlier, DHIS2 provides a toolkit designed for COVID-19 surveillance in a manner where it could be customised for specific country workflows (DHIS2 2021b).
Where vaccine distribution plans already exist, donors can encourage governments to publish these in accessible formats to the public to minimise the potential for corruption and abuse.
Access to information on the acquisition and pricing of vaccines
Beyond identifying and targeting priority populations, access to information can be a powerful tool to ensure accountability and fairness in the rollout of vaccinations more generally.
The Open Government Partnership (2021) reveals that many countries are not disclosing even the most basic data on vaccinations in a timely or regular manner. To deal with this problem Transparency International (2021) has developed a toolkit that sets out five questions every government ought to proactively answer about COVID-19 vaccines:
- Which vaccines has the government acquired?
- How many doses of each vaccine have been secured?
- When will the vaccines be delivered to everyone?
- How much is the government paying for a dose of each one of the vaccines secured?
- Has the government produced a single website with all the information on the vaccination plan including timelines, coverage, financial resources and contracts?
In response to the 150% inflation of Covid-19 vaccine prices in the country, Transparency International Pakistan is using these five questions to liaise with the government to make such information publicly available (Transparency International Pakistan 2021). Donors could adopt a similar approach by encouraging aid-recipient governments (as well as their own home governments) to proactively publish this information as the first step to track rollout and help identify irregularities.
Transparency in the negotiation for vaccine prices has been a matter of discussion for several years. Pre-Covid, in 2014, WHO launched the Market Information for Access to Vaccines (MI4A), an initiative to make vaccine product, price, and procurement information available to enhance vaccine price transparency (WHO 2019b). The database created by MI4A has supported lower- and middle-income countries to negotiate for affordable prices and strengthen their access to affordable vaccines (Sciacchitano and Bartolazzi 2021).
However, the issue is still far from being resolved. As mentioned earlier, confidentiality clauses have proliferated as governments compete to acquire vaccines. The result has been that some countries, including South Africa and Hungary, are reportedly paying substantially more than other countries for the same product. At the international level, even the EU – which publicly recognises the importance of transparency – is refusing to disclose information on pricing and negotiations (Sciacchitano and Bartolazzi 2021).
Confidentiality may be necessary in some cases to protect proprietary information about vaccine formulas and other patent considerations. However, Transparency International (2021) argues that confidentiality clauses should not be used to deny the public their right to information on essential questions, such as prices paid for with public resources, the quantity of vaccines purchased, contractual conditions and the distribution timeline.
When it comes to transparency in procurement and public financial management, donors ought to encourage and incentivise aid-recipient governments to continue to use models such as open contracting and e-procurement for the Covid-19 vaccines. As the Open Government Partnership (2021) states, open procurement processes “ensure value for money, reduce corruption and boost public trust” (Falla 2021).
Particularly in light of mounting evidence of unfair pricing strategies and extortionate demands placed by pharmaceutical companies on states, such as demanding sovereign assets as collateral and exemptions from financial liability, donors have a strong case to make that open contracting is in states’ own interest (Corporate Europe Observatory 2021; Davies et al. 2021)
Donors could look to replicate the existing transparency standards of the IMF Rapid Credit Facility (RCF) and Extended Credit Facility (ECF), whereby IMF support comes in exchange for structural benchmarks related to strengthening public financial management (PFM) and procurement systems (IMF 2020; IMF 2021). IMF conditionality standards and programme designs are tailored to reflect members’ circumstances. For example, an IMF review (2019) found that fragile states had relatively more conditions relating to PFM and revenue administration (IMF 2019).
Country cases
Argentina expanded health contracting disclosures to include agreements signed with laboratories, open data on individual purchases, and a list of most-procured medications (Pousadela 2020).
Liberia committed to disclose supply chain management decisions and updates, including on emergency procurements during the pandemic (OGP 2020).
Awareness raising campaigns
Finally, donors could provide financial support to public information campaigns about vaccination in lower- and middle-income countries, especially in countries where low levels of trust in governments translate into fewer people signing up for Covid-19 vaccination.
These campaigns could involve working in tandem with NITAGs and Ministries of Health to publicise distribution plans and to ensure that at-risk groups and those considered vulnerable in hard-to-reach areas are made aware of their entitlements to vaccination and know where they can get vaccinated.
Leverage donor influence on COVAX partners
The Coalition for Epidemic Preparedness Innovations (CEPI), which is part of the COVAX platform to ensure equitable Covid-19vaccine rollout has been criticised for a lack of transparency (Usher 2021). Another criticism levelled against COVAX is that it has not ensured that data and technology around the vaccine is shared with low-income country manufacturers (Ravello 2021).
Observers and health experts are demanding more transparency in CEPI’s operations, particularly grant agreements with vaccine developers and for CEPI to step up monitoring of pharmaceutical companies’ deals with governments (Usher 2021). Donors, being key stakeholders in COVAX’s Advance Market Commitment programme, could seek to leverage their position to ensure that such demands for transparency translate into meaningful improvements.
The heads of key donor countries, including the USA and Sweden, have expressed the importance of COVAX when it comes to equitable Covid-19 vaccine access (WHO 2020). Donors could attempt to build on this momentum to overcome the collective action problem by lobbying governments (including their own) to use the COVAX pooled procurement mechanism as well as multi-donor funds, such as the Global Fund, that are believed by observers to have robust corruption prevention and integrity management functions in place (Steingrüber et al. 2020).
In such cases, ensuring the integrity of donor governments’ own contracting processes is important for donors to act as a credible voice when it comes to calling for equitable vaccine rollout in lower- and middle-income countries. The Biden administration has come forward in this regard by making vaccine distribution transparency a priority (Buble 2021).
Donors could also encourage leading actors to mainstream anti-corruption concerns into their guidance material aimed at helping countries to develop vaccine deployment plans. In particular, the WHO’s Guidance on Developing a National Deployment and Vaccination Plan for COVID-19 Vaccines, the WHO’s Pandemic Influenza Preparedness and Response Guidance document, and Gavi’s reference document COVAX: The Vaccines Pillar of the Access to Covid-19 Tools Accelerator: Structure and Principles would benefit from greater consideration of corruption risks and integrity mechanisms (Kirya 2020).
A recent report by Kohler and Bowra (2020) on exploring anti-corruption, transparency and accountability in WHO programmes, the United Nations Development Programme (UNDP), the World Bank Group and the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) found that there has been a clear increase in the volume and scope of such measures being implemented by these international organisations in recent years. However, it also cautioned that the efficacy of these measures translating to delivery on anti-corruption remains unclear (Kohler and Bowra 2020). A few areas to be noted in anti-corruption compliance for the aforementioned organisations are as follows (Kohler and Bowra 2020):
- WHO: the internal auditor to the World Health Assembly (WHA) reported that operating effectiveness of controls in WHO country offices dropped significantly from 83% in 2017 to 60% in 2018.
- UNDP: in 2018, a total of 520 cases concerning fraud, corruption and misconducted were reported; 54% of these reported cases concerned financial irregularities, such as procurement fraud, theft and embezzlement.
- Global Fund: it has witnessed a change in trends from largely procurement fraud in 2014–2015 to a diverse range of fraud and corruption in 2018.
- World Bank: the annual report of its sanctioning system found that of the total cases opened in 2019, 71% were related to fraud, 35% to corruption, 33% to collusion, 2% to coercion, and 6% to obstruction.
Given the relevance and importance of these organisations in the health sector, especially in the context of the ongoing pandemic, donors could encourage improvements in the implementation of anti-corruption controls on the ground.
Donors could also call on Gavi and other COVAX partners to move beyond a focus on ex-post measures to tackle corruption, such as audit and investigation,c44c6be42371 and invest in ex-ante prevention measures, such as risk assessments, management and mitigations. The benefits of ex-ante reviews are demonstrated by a World Bank evaluation of more than 1,000 investment cases which showed that as many as 80% of the cases that conducted a thorough feasibility study and secured “quality at entry” were successful, whereas only 35% of those with poor preparation were successful (Samset and Christensen 2015).
Strengthen oversight bodies
Oversight bodies serve key monitoring, audit and sanctioning functions (Jenkins et al. 2020). As such, both pre-existing and specialised bodies tasked with Covid-19 vaccine distribution ought to be supported in terms of their mandate, functions and capacity to enable them to identify and mitigate corruption risks (Jenkins et al. 2020).
To help develop the capacity of relevant oversight bodies to deal with the specificities of the health sector, donors could seek to foster collaborations between oversight bodies and relevant sectoral initiatives, such as the Coalition for Accountability, Transparency and Anti-Corruption in Health (CATCH) (Steingrüber 2020).
UNODC (2020) states that to empower oversight bodies to identify red flags related to Covid-19 vaccine distribution in real time, their functions should include the “capability to monitor the emergency disbursements of funds, the purchase of vaccines, and the distribution of vaccines and related processes”. The World Bank has recommended that supreme audit institutions be helped to use ICTs to remotely access government systems and continue with audits, including real-time rolling audits. For example, based on the experience of the widespread fraud encountered during the Ebola outbreak, the International Federation of Red Cross and Red Crescent Societies (IFRC) has put in place a full-time auditor to monitor its Covid-19 programming (Thorp 2020).
Part of this may involve the development of open vaccine distribution tracking mechanisms, which allow for regular updates on the national distribution of vaccines, where they are being distributed to, and who is receiving them. This information can be cross-checked and triangulated with reports from communities, patients’ rights groups and health centres to uncover any irregularities in the storage, transportation and delivery of vaccines.
Donors could consider funding measures designed to improve security in storage and tracking of vaccines in transit, such as GPS and geo-tagging systems (UNODC 2020). Spot-checks by oversight authorities may also reduce incentives for unscrupulous actors to embezzle funds.
Such tracking systems can be used by oversight bodies to monitor distribution performance, and to put pressure on duty bearers to increase transparency and accountability in distribution. As well as providing technical assistance and financial resources to support the development of tracking systems, where feasible, donors could work with aid-recipient governments to link this data to national health management information systems, allowing vaccines to be tracked throughout the system to the point of delivery. Notably, DHIS2 have developed a plugin for COVAX to keep track of vaccination activities and perform daily stock management (DHIS2 2021a).
Country cases
South Africa: the inter-ministerial committee has assessed potential corruption risks and counter measures throughout the value chain of the vaccine programme. This risk assessment has been supplemented with lessons learned from the experience of procuring personal protective equipment, where there was widespread non-conformity to product quality standards. The procurement of vaccines has been centralised in the department of health, and provincial administrations are required to choose from pre-selected service providers and distribution plans. For added oversight, the auditor-general has been granted access to the non-disclosure agreements entered into with manufacturers and suppliers. Vaccine administration is to be done only via registered centres for vaccination that are publicised. Daily reconciliation of vaccine doses at inoculation centres would be done for effective monitoring against theft and other leaks. Finally, whistleblower and anti-corruption units in the presidency and the Special Investigation Unit have been put on alert to detect any corrupt activities in vaccine rollout (Maqhina 2021).
Malawi: in response to the public outcry over endemic corruption in the management of Covid-19 funds, the ombudsman established a public service system review task force. The mission of the task force is to review allowances, procurement, contracts and conditions of service in the implementation of the National Covid-19 Preparedness and Response Plan (Office of the Ombudsman, Malawi 2021).
Peru: The country has empowered the supreme audit institution to conduct concurrent monitoring when processes are being implemented as opposed to just ex-post. For example, during the procurement process, it will monitor activities to prevent misuse and to help implement timely corrective action under the framework of the Covid-19 emergency plan (Wendling et al. 2020).
Nigeria: acting on the statement of the presidential task force dealing with the pandemic, which reported on the confiscation of 3,000 vials of fake COVID-19 vaccine, the customs service has only allowed Nnamdi Azikiwe International Airport in Abuja to be a port of entry for Covid vaccines (Federal Ministry of Health, Nigeria 2021).
Colombia: the comptroller-general’s office uses OCEANO, an analytics platform that cross-checks information from the e-procurement database to detect possible irregularities. This tool has revealed suspicious links between certain companies and some provincial governors and city mayors, which led it to identify cost overruns in health emergency related contracts (Economia Colombiana 2019).
In-country partnerships with international and non-government organisations
When it comes to distributing vaccines in difficult governance settings, donors may choose to partner with international or non-governmental organisations that have deep contextual knowledge of the operating environment and may enjoy high levels of trust and perceived legitimacy among the population. In certain contexts, populations tend to trust non-profits, charities and civil society organisations (CSOs) more than their own governments (Charity Commission and Populus 2016; Chronicle of Philanthropy 2015).
While this should not serve as a pretext to absolve national governments of their responsibilities as primary caregivers, donors may find that bodies such as UNICEF have existing vaccination schemes in fragile settings, as well as experience in maintaining the cold chains necessary for vaccine roll out. In addition, UN agencies or bodies such as the Global Fund may have better developed integrity management systems and more effective monitoring and sanctioning regimes than local government bodies, making it more likely that corrupt practices will be identified and stopped. However, when possible, donor’s engagement with non-state actors should aim to include governments to enhance their capabilities in the long term. Otherwise, excluding them can come at the expense of projects’ sustainability.
Country case
Democratic Republic of Congo: COVAX vaccines in the DRC are in the custody of UNICEF. UNICEF is helping with the logistics of delivering the vaccines through the cold chain including the transport of injection materials and protection materials (UNICEF 2021).
Third-party monitoring
IFRC: the World Bank and the IFRC have signed an agreement for the independent monitoring of Lebanon’s Covid-19 vaccination campaign. Under this agreement, IFRC, acting as the third-party monitoring agency (TPMA), will be in charge of independently monitoring the compliance of the vaccination deployment with national plans, international standards and World Bank requirements to ensure safe handling of the vaccines, as well as fair and equitable access to all (World Bank 2021).
IFRC’S oversight and supervision is to cover Covid-19 vaccine supply chain management as well as vaccine administration at vaccination sites from the technical, environmental and social safeguard perspectives. This includes but is not limited to storage, stock and temperature maintenance across the supply chain, service delivery at vaccination sites, eligibility of vaccine recipients and capturing client perspectives and feedback (World Bank 2021).
In addition to the TPMA, the World Bank has established, in consultation with other international actors, joint monitoring committee to engage in the monitoring of the vaccination process, identify measures to enhance the quality of the campaign, and ensure joint advocacy throughout the process based on findings from the TPM and other sources (World Bank 2021).
In Colombia, the government has committed to establishing citizen audits of government expenditures on Covid-19 related measures (OGP Colombia 2020).
Role of civil society in monitoring rollout
A thriving civic space is a powerful counterweight to corruption. CSOs can play a pivotal role in equitable vaccine rollout by raising awareness to various groups’ entitlements while simultaneously acting as accountability mechanisms. Recognising their role, Asian Development Bank (ADB) has adopted an approach to mitigate the impact of Covid-19 through community led interventions by providing technical assistance to partner CSOs on (ADB 2020):
- community-based mitigation and prevention activities
- social protection for vulnerable communities, including elderly care
- economic support for those with livelihoods affected by Covid-19
Past experiences have shown that there are several proven ways for CSOs to complement action by governments and donors in vaccination programmes (Bhargava 2021), such as:
- assist in community outreach to educate and counter misinformation
- assess the extent of and reasons for vaccine hesitancy, and then design tailored messages to overcome it
- identify those who might not be covered in vaccination rollout due to various barriers (e.g., mobility, language, identity, remoteness, etc.)
- monitor compliance with vaccine allocation criteria and adverse reaction protocols, identify and close vaccine service delivery gaps and administer vaccines when authorised
- monitor integrity in procurement and distribution of vaccines and associated supplies (gloves, mask, syringes etc.)
- track vaccine delivery including delayed and interrupted supplies
- work with budget, audit, ombudspersons, and anti-corruption agencies, using participatory practices, to help them frame the scope of audits and to develop a database on alleged corruption cases for investigations
Such projects and community participation networks could be leveraged by donors and governments to monitor vaccine rollout by promoting the active participation of CSOs in monitoring the prioritisation of recipients, the procurement of vaccines, and the flow of emergency funds for vaccine programmes.
Indeed, donors could seek to encourage the mobilisation of existing CSO networks and community-based organisations to ensure that the right people are being vaccinated. In countries like Malawi, for instance, village health teams are already in use for tuberculosis and HIV/AIDs managements. Given that the main issues in such monitoring initiatives is counting (the number of vaccines expects vs the number delivered, how many residents need a vaccine etc.), national census enumerators or those who conduct health surveys may also be useful partners. They could be deployed to help identify at-risk groups and monitor their vaccination rates as they may be more aware of these groups’ specific needs and conditions.
Such approaches have the potential to help overcome situations in which national health information management systems are underdeveloped and people lack formal identification, or where internet penetration is very low.
Finally, donors could also consider deploying or engaging country based observers, based on the Global Fund’s local fund agent model. These people “monitor grant implementation and progress on behalf of the Global Fund, complete a biweekly survey online to help identify potential risks and disruptions to programs” (The Global Fund 2021). While the tool cannot provide a comprehensive assessment of corruption risks in a country, it can act as an early warning system, and when triangulated with other data sources, help identify red flags that may affect vaccine rollout.
CSO intervention examples
Community radio: in Bangladesh, community radios are being used by CSOs to broadcast awareness raising campaigns about COVID-19 vaccination and to counter disinformation. The programmes include news on immunisation at the local level, interviews and experiences of those who have been vaccinated (BNNRC 2021).
Demands for transparency and accountability in vaccination processes: Keeping track of corruption in COVID responses by monitoring missing relief funds, the Civil Society Legislative Advocacy Centre in Nigeria demanded transparency in the COVID-19 vaccine delivery process from the Nigerian government (Vanguard 2021). In a public statement, the organisation also called for the need to investigate and prosecute those who diverted medical materials and money meant for Nigerians during the COVID crisis (Ewepu 2021).
Monitoring tool to track vaccine rollout: the Transparency International chapter in Honduras (Asociacion por una Sociedad mas Justa) has set up an online monitoring tool to track the origin, allocation, and distribution of COVID-19 vaccines. The site is called Vacunas abiertas (Open Vaccines) (Vacunas Abiertas 2021).
Reporting channels to document malpractice and corruption for later audit and ex-post accountability
Audit, oversight, reporting and monitoring mechanisms are key to ensuring accountability, even if this takes place after the initial emergency has subsided (Jenkins et al. 2020). One of the steps that donor agencies can take is to earmark funds in their Covid-19 programmes for thorough ex-post audits and widely communicate this decision, while also appointing a records custodian (Jenkins 2020). Donors can also emphasise the importance of civic space and whistleblower protection to those raising voices around corruption in Covid-19 vaccine processes (Jenkins et al 2020).
Whistleblowing, reporting and grievance channels are particularly important to identify and resolve suspected malfeasance in the vaccine rollout. Given that women are crucial to vaccine uptake6a2fdd0b0a20, donors could highlight the importance of gender sensitivity in corruption reporting and whistleblowing (Harman et al. 2020; Zúñiga 2020).
Reporting examples
Philippines: local government authorities are required to prepare monthly reports on the use and implementation of COVID-19 related special grants. The reports are required to be published on their respective websites and posted at a minimum three of conspicuous public places in the community. The chief executive of the local authority is required to send a written notice informing the Congress and relevant congressional committees of the publication of reports (Wendling et al. 2020).
Palestine: TI Palestine is campaigning for vaccine transparency by asking witnesses to come forward and report any practices such as wasta, nepotism and favouritism in the distribution of the vaccine via toll free numbers (TI Palestine 2021).
Transparency International’s (TI) Advocacy and Legal Advice Centres (ALACs): since January 2020, TI ALACs have supported more than 1,800 people who contacted them to report corruption and seek assistance for corruption issues related to COVID-19 (Transparency International 2021c).
Global Fund: the Office of the Inspector General (OIG) reports on all of Global Fund’s activities in the interests of transparency and accountability. In 2020, whistleblowers represented half of the total reports received by OIG, with 16% of those coming from Global Fund secretariat staff. There has been an increase in both implementer and local fund agent reporting. Whistleblowers tend to use the inspector general email account and the third-party incident reporting channel accessible via the I Speak Out Now website (OIG 2020). The I Speak Out Now website also offers an e-learning platform where Global Fund partners can find out more about the different kinds of wrongdoing, case studies and tools to counter corruption in their programmes (Global Fund 2017).
Trade-offs: expediency vs integrity
Corruption is occasionally seen as a cost of doing business in crisis situations, especially where there is a perceived trade-off between expediency and due diligence. Yet anti-corruption procedures and accountability mechanisms are some of the best instruments to ensure that humanitarian assistance is being used effectively and governments’ and donors’ objectives are achieved.
Ultimately, well-designed internal controls and emergency protocols are not simply additional bureaucracy but measures that allow donors to “maintain control and effectiveness even when moving at high speed” (Transparency International 2014).
In the short-term, ensuring the quick roll out of vaccines versus monitoring requirements may require some trade-offs. Jenkins et al. (2020) provide an overview of concrete measures that donors can take to minimise the risk of corruption. Among others, these include:
- conduct risk-based due diligence where possible, prioritise partners presenting higher risks
- if ex-ante due diligence is not possible due to urgency, be sure to complete due diligence processes after the first disbursement of funds
- continue to issue contracts and document transactions, as well as document exceptions to standard procedures, even after contracts are signed.
- set aside specific and substantial resources for ex-post evaluation and audit, and widely communicate this decision to deter potentially corrupt behaviour
- consider offering financial incentives to those who report misappropriation of donor funds
- support efforts by national health ministries to establish transparently appointed Covid-19 oversight taskforces that include representatives from the national audit office, anti-corruption experts, experts from civil society and similar bodies. Encourage national governments to empower these bodies to monitor pandemic-related financial allocations.
- use clear, objective and transparent criteria to identify intended beneficiaries
- ensure that those eligible for assistance are made aware of the nature and level of support they are entitled to, and the method by which this will be delivered. Online platforms, social media and community radio may be valuable channels to communicate this information.
- consider establishing a dedicated fund to ensure civil society and journalists are able to continue their work
While the unprecedented situation created by the pandemic has created significant corruption challenges, it also presents an opportunity to create better healthcare and oversight systems that prioritise the most vulnerable in society, are based on robust data, and strengthen participatory monitoring.
The goal of strengthening national vaccination processes ought not be limited to addressing current corruption risks alone but contribute towards achieving universal health coverage.
Making this ambition sustainable will nonetheless require careful consideration of how best to embed measures to counter graft, corruption and mismanagement into the design of healthcare policies and programmes. In the longer term, it would also demand that donors develop contingency plans for expedited oversight processes and flexible yet robust integrity mechanisms able to withstand future health emergencies.
- A health information system (HIS) refers to a system designed to manage healthcare data. This includes systems that collect, store, manage and transmit a patient’s electronic medical record (EMR), a hospital’s operational management or a system supporting healthcare policy decisions (Brook 2020).
- DHIS2 is an open source, web-based platform most commonly used as a health management information system (HMIS).
- Vaccine cold chains are a global network of cold rooms, freezers, refrigerators, cold boxes and carriersthat keep vaccines at the right temperature during each link on the long journey from the manufacturing line to the syringe (Path 2021).
- Sexual extortion or “sextortion” occurs when those entrusted with power use it to sexually exploit those dependent on that power. It is a gendered form of corruption (Feigenblatt 2020).
- Value chain assessments adapted from Selinšek (2015)and Jenkins and Chêne (2018).
- Vertical forms of accountability are where a subordinate usually reports to a superior, whereas horizontal accountability arrangements address peers, equals, stakeholders or concerns outside of the hierarchal relationship (Schillemans 2008).
- NITAGs are multidisciplinary groups of national experts responsible for providing independent, evidence-informed advice to policymakers and programme managers on policy issues related to immunisation and vaccines (WHO 2019).
- Based on the Gavi Alliance Audit and Investigations: Terms of Reference.
- Some scholars suggest that the delivery and facilitation of COVID-19 vaccines will disproportionately depend on the unpaid labour of women (Harman et al. 2020).