Health sector corruption: A matter of life and death
For decades, donors have worked to strengthen anti-corruption, transparency, and accountability institutions in partner countries, but the development of specific approaches to address corruption in the health sector (and in other public service sectors) is more recent. A first wave of policy and programme guidance for the health sector emerged around 2010, including the original U4 Issue on the topic, Addressing corruption in the health sector: Securing equitable access to health care for everyone.aa97e2f38721 Since then, anti-corruption initiatives specific to health have been pursued around the world. At global level, meanwhile, the Sustainable Development Goals include commitments on universal health coverage and on good governance and transparency. In light of such changes, U4 has updated the original U4 Issue to provide guidance for donors on anti-corruption, transparency, and integrity approaches in health at the international and national levels.
Impact of corruption on health sector performance
Corruption in the health sector can make the difference between living and dying, especially for poor people in developing countries. A 2011 study analysing data from 178 countries estimated that the deaths of approximately 140,000 children per year could be indirectly attributed to corruption. Child mortality correlated more strongly with national corruption levels than with literacy, access to clean water, or even vaccination rates.1eb036cf09a3 In another study, antimicrobial resistance was found to be linked as much to national corruption levels as to antibiotic use.995fa6f1199c And the reduction of AIDS deaths has been significantly slower in countries with higher corruption levels.dc248b271dbd
Corruption in the health sector has severe consequences for access, quality, equity, efficiency, and efficacy of health care services – the five dimensions of health system performance.
Access to health services can be seriously affected by absenteeism of medical staff. Estimated rates range from 19% to 60% in low- and middle-income countries, with more qualified staff like doctors and pharmacists showing higher rates of absenteeism than less qualified staff.c68903ceccd0 Another barrier to access is demands for informal payments or bribes in exchange for services that citizens are entitled to receive for free. The incidence of bribes in direct interactions between citizens and health service providers varies widely, from 1% to 51% at global level, with higher levels in Africa, Central and Eastern Europe, and the Middle East/North Africa, and lower levels in Western Europe and the Americas.abf83b7627dd Theft, embezzlement, and bribery also affect access to needed medicines, equipment, and supplies. For example, in Togo a government audit discovered that a third of the anti-malarial medicines provided by the Global Fund to Fight AIDS, Tuberculosis and Malaria, worth over US$1 million, had been stolen.251c4fcad6a2
Quality of care and medical drugscan be severely compromised by bribes, kickback schemes, and fraud. Countries such as Tanzania, Uganda, and Ukraine have recognised corruption as one of the major barriers to providing quality health services.da0edbd5b026 Patients may be charged for diagnostics and treatments that are fake or substandard or were not performed at all. Additional problems include kickback-driven referrals and unnecessary procedures. A study by the World Health Organization (WHO) found that worldwide, 6.2 million unnecessary caesarean sections are performed every year, 2 million of them in China alone.49f6a06aa444
Good-quality medicines may be unavailable due to drug theft, stockouts, or extortion. Profiteers use corrupt schemes to avoid government regulation of drugs. Globally, 10% of all drugs are believed to be fake, while in some African countries the figure can amount to 50%.afe4158775ce Counterfeit drugs can lead to severe illness and death, as well as to the spread of drug-resistant viral or bacterial strains within and across countries.
The effect of corruption on equity is a great concern. Families fall into deeper poverty when they are forced to sell assets or go into debt in order to pay bribes for health services that they should have received without charge. Evidence shows that bribes are regressive, imposing a major burden on poorer households. In Peru, the poorest households spent 15% of per capita income on informal payments in general. Economic shock from illness was the most common cause of falling into poverty in Vietnam, affecting 3 million people in 2010.458fbe80a083
Corruption has enormous effects on the efficiency of the health sector, in particular the availability and use of scarce resources. Globally, an estimated 7% of health spending, amounting to more than $500 billion per year, is lost to corruption and fraud.0e3ce2acd3fa Even in Western European countries, the United States, and Canada, the losses are high, estimated at up to 10% of public health expenditure in Germany, 56 billion euros annually in Europe, and $75 billion in the United States for Medicare and Medicaid payments alone. The British Centre for Counter Fraud Studies found that ‘since 2008, losses as a result of corruption have increased by 25% worldwide and even by 37% for the National Health Service in the UK.’8f6f26891d96
Aggregated estimates for developing countries are scarce, but the following examples help illustrate severe efficiency losses. A study of 64 countries found that corruption lowered public spending on education, health, and social protection. In Chad, local regions received only a third of centrally allocated resources; in Cambodia, 5%–10% of the health budget was lost at the central level; in Tanzania, local or district councils diverted up to 41% of centrally disbursed funds; and in Uganda, up to two-thirds of official user fees were pocketed by health staff.d0baddaf0d2a Corruption and lack of transparency also affects drug pricing. In Vietnam, health facilities paid eight times and patients 46 times the international reference price for certain brand-name drugs, and two or 11 times, respectively, for generics; meanwhile, drug costs constitute 50% of the Vietnamese public health budget.394c8a4b5d6f
In terms of efficacy, corruption in the health sector has a corrosive impact on the population’s health, as illustrated by the examples noted earlier. According to the Transparency International (TI) Health Initiative, ‘Multiple studies have found that high levels of corruption are linked to weak health outcomes, and there is strong evidence to suggest that corruption significantly reduces the degree to which additional funding for the sector translates into improved health outcomes.’ In other words, pouring more money into highly corruption-prone health systems will not achieve the intended health goals. More broadly, corruption in the health sector erodes the legitimacy of, and public trust in, government institutions. The same TI report continues, ‘Political stability and efforts to contain epidemics are undermined because citizens encountering corruption at their local clinic lose faith in the state’s willingness and ability to provide basic services.’bd9c88862a9e
Finally, corruption is an obstacle to the long-term goal of achieving universal health care (UHC). The World Health Organization has identified good governance as a ‘critical element’ of efforts to achieve UHC.4c5464fa730f Globally, corruption in the health sector is estimated to cost more money than what would be required to achieve UHC. As noted above, an estimated $500 billion per year in public health spending is lost to corruption. In order to achieve UHC, an additional $370 billion per year would be needed until 2030, with international development funding required to cover $17–$35 billion.6150756f4f4e By this logic, the funds lost to corruption in the health sector globally could essentially fill the implementation gap for UHC.
The health sector’s vulnerability to corruption
A number of factors make health systems particularly susceptible to corruption. They include the vast quantities of resources flowing through these systems; the high level of uncertainty; asymmetry of information; the large number of actors; the complexity and fragmentation of national health systems; and the globalised nature of the supply chain for drugs and medical devices. These factors, explained briefly below, hinder transparency and accountability and create systematic opportunities for corruption, regulatory capture, and undue market pressure.
Resources spent in the health sector globally and at country level offer lucrative opportunities for abuse and illicit gain. As noted above, annual global spending on health is estimated to exceed $7.5 trillion in 2016.06dd5588a3f5 Health spending ranges from around 4% of gross domestic product in low-income countries to more than 15% in countries of the Organisation for Economic Co-operation and Development (OECD), with a rising trend.ae45967da333
Uncertainty regarding the effectiveness of medical treatments and the inability to predict who will fall ill, when, and with what kind of illness makes health markets distinct from others, leading to inefficiencies and scope for abuse. The poor functioning of health markets makes it difficult to set standards for accountability and to discipline health care providers for poor performance. Consumer choice is not a good regulator: particularly in developing countries, patients often cannot shop around for the best care, given distance, public service delivery monopolies, and limited availability or high cost of private care.
Similarly, the health sector is characterised by a high degree of information asymmetry. Information is not equally available to all actors. This makes it difficult to fully monitor the actions of different actors, hold them accountable, detect abuses, and assign responsibility. Patients lack information to judge medical decisions made on their behalf or to assess the correctness of a bill, and the discretion given to providers puts patients in a weak position if providers choose to abuse their position. Even insurance auditors may have a hard time evaluating whether a bill is correct and the services provided were necessary. Asymmetry of information also affects decisions related to procurement of medicines and medical devices. Pharmaceutical company representatives know more about their products than do the doctors who prescribe them, and regulators are hard pressed to ensure the quality of drugs and medical equipment. Policy and regulatory issues related to benefit packages, drug prices, and market access of new health technologies, among others, are also affected.
The large number of dispersed actors involved in health systems exacerbates these difficulties. The relationships between medical suppliers, health care providers, health service payers, and policy makers are often opaque, making it difficult to detect conflicts of interest that can lead to policy distortions. Health service delivery is often decentralised, making it difficult to standardise and monitor service provision and procurement.
National health systems are complex and often fragmented, with different sub-systems attending to the health needs of different populations. For example, there may be sub-systems for public sector employees, for workers in the formal economy with labour contracts, for the military and/or police, and for the informal sector and/or the poor. Most countries’ systems involve a combination of public and private health care providers (with the latter often far less regulated than the former), and there may also be a combination of public and private health insurers. The multiple logics of these sub-systems and the different legitimate and illegitimate interests of the various actors provide opportunities for corruption and for regulatory and policy capture.
Finally, the global nature of the supply chain for drugs and medical devices allows for undue market pressure, information manipulation, regulatory capture, and abuse. This relates to the globalised nature of the pharmaceutical and health care product industries, their enormous size, and the inherent conflict between their legitimate business goals and the medical needs of the public.
Because these various factors create vulnerability to abuse, health care is among the most heavily regulated sectors in most countries. However, powerful interest groups frequently try to capture the regulators and influence their decisions through a variety of strategies, including undue influence, bribes, and complex kickback schemes.
Identifying and punishing corrupt practices in health remains difficult. The lines between inefficiency or unintentional misconduct, on one hand, and unethical behaviour, intentional abuse, and criminal behaviour on the other can be blurred, and abuses may be hidden behind apparent inefficiencies. Also, the imperative to save lives at all costs may impede frank discussions among government actors and development partners about corruption in the health sector. But experiences from around the world have shown that it is possible to begin a dialogue about these problems and develop strategies to address them (see Annex 1).
Understanding corruption in the health sector
The term ‘corruption’ means different things to different people, and there is no universally accepted definition. Transparency International defines corruption as ‘the abuse of entrusted power for private gain.’d6573c388b74 Those with entrusted power include public sector officials (whether appointed or elected) as well as officials and staff of private companies, international organisations, and civil society organisations.587a3d3516d8
The principal international treaty on corruption, the United Nations Convention against Corruption (UNCAC), does not define corruption as such. Rather, it enumerates specific acts of corruption, including bribery and embezzlement, influence trading, abuse of function, illicit enrichment, money laundering, concealment, and obstruction of justice. However, jurisdictions differ in terms of which practices are or are not criminalised. One of the starting points for addressing corruption in any country is to know how it is defined in the country’s own constitution and laws.
How does corruption manifest itself in the sector?
The various types of corruption find many manifestations in national health systems. Different health systems are prone to different types of corruption, and the risks for abuse depend in part on how funds are mobilised, managed, and paid.
Integrated systems are ones where the public sector finances and directly provides health care, as is common in developing countries. They tend to be particularly vulnerable to large-scale diversion of funds at the ministerial level, as well as in financial flows from the national to the subnational levels. Bribes and kickback schemes in procurement, illegally charging fees to patients, diverting patients to private practice, and absenteeism are also common. Finance-provider systems separate public financing from health service provision, and are more common in middle-income countries. They tend to be particularly vulnerable to fraud in billing government and insurance agencies. They can also suffer from excessive or low-quality medical treatment, depending on the payment mechanism, as well as regulatory capture and conflicts of interest. State and policy capture, and corruption in the drug supply chain, procurement, and appointments, can occur in both types of system.4a0a85792702
Case studies of health sub-systems for the poor in Colombia and Peru provide an illustration of how corruption can take different forms across different health systems (Box 1).
Box 1: Corruption in the Colombian and Peruvian health sub-systems for the poor
In 2011, the United Nations Development Programme (UNDP) commissioned a study to explore the main vulnerabilities to corruption in the national health sub-systems of Latin America that provide services to the poor.* The results from Colombia and Peru present interesting insights.
First, there are basic structural differences between the two systems. Colombia’s subsidised health insurance system for the poor separates payments from providers and features regulated competition among a mix of public and private health insurers and providers. The Peruvian sub-system serving the poor is managed by the Ministry of Health and relies on direct, public provision of health services by public staff.
The Colombian system is highly decentralised in its authority, functions, and financing, the result of a major health reform started in the 1980s. By contrast, the Peruvian system remains substantially more centralised. Furthermore, Colombia has a progressive financing insurance structure, while Peru still depends heavily on out-of-pocket payments by users, the most regressive form of health care financing.
The study found that in Colombia, the main vulnerabilities related to fraud and corruption in claims processing and beneficiary affiliation. These are areas of vulnerability that do not exist in integrated public provision systems. Decentralisation of the subsidised system, in particular in the administration of funds, seemed to imply a decentralisation of corruption risks. At the same time, decentralisation allowed Colombia to achieve high health insurance coverage. Finally, vulnerability to policy and regulatory capture clearly affected the whole system in Colombia, including the regulatory and supervisory bodies themselves.
Peru, meanwhile, showed notable vulnerabilities in the area of human resources. Key problems included provider absenteeism; redirecting of patients to private practice instead of treating them for free; and the ‘buying’ of jobs and promotions. The management of drugs and supplies, as well as asset management in health establishments, also surfaced as particularly subject to abuses in Peru but not in Colombia. In addition, stewardship by the Peruvian Ministry of Health was perceived as weak, especially with respect to its controls on spending.
In both countries, procurement of drugs and medical supplies continued to be susceptible to corruption and undue influence despite reform efforts. Political interference in the nomination of hospital directors, which is supposed to be based on merit, was pervasive, with serious consequences for hospital performance. And in both countries, corruption was perceived to be higher in the other health sub-systems that serve the richer part of the population and people with formal employment, perhaps in part because they involve larger flows of resources.
Several insights can be gleaned from the Colombia-Peru comparison. First, the emergence of corruption scandals should not lead to hasty conclusions that one system is more prone to corruption than another. They simply have different dynamics and loci that attract corrupt activity. Second, decentralisation is not a ‘silver bullet’ for increased transparency and accountability. But there is no evidence, either, that centralised systems are necessarily less corrupt. Third, laws, norms, regulatory processes, and health sector oversight agencies are valuable targets for capture, but little attention has been paid to these issues. And fourth, an integral strategy of internal and external controls, with strong stewardship by the national health authorities, is essential but often lacking.
* Hussmann (2011b).
To assess the vulnerabilities in a given health system or sub-system, one can start by examining the roles and relationships among different players and understanding the ‘rules of the game.’ The players can be classified into five broad categories:
- Government regulators (parliaments, health ministries, and specialised health regulation, oversight, or public health agencies)
- Payers (public social security institutions, private insurers, government health funds)
- Providers (public and private hospitals, doctors, pharmacists, NGOs, faith-based organisations)7c3616f0eef2
- Consumers (patients)
- Suppliers (medical equipment, pharmaceuticals, construction, ambulances)
Figure 1 illustrates typical corruption risks arising from relationships between these main actors. Most publicly available research on these risks and possible mitigation strategies focuses on the service delivery level, that is, on interactions between providers and users, as well as on the pharmaceutical and health product supply chain. The risks of policy, regulatory, and institutional capture, and of corrupt interactions between payers and providers, tend to be under-researched, even though they have great impact on overall health system performance.
Figure 1: Examples of corrupt practices among different health sector players
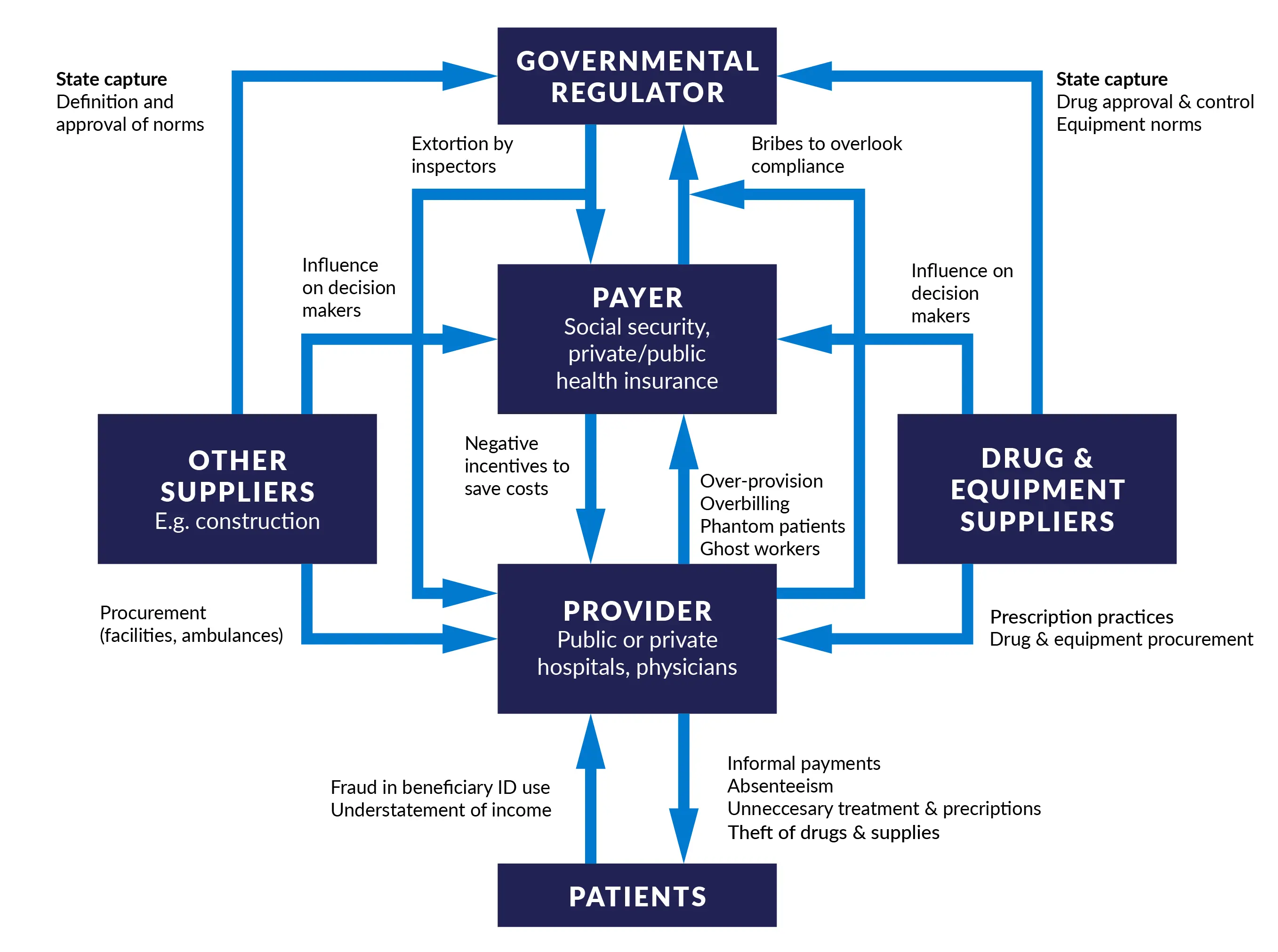
Source: Adapted from Savedoff and Hussmann (2006).
Corruption used to be framed mainly as misconduct or criminal behaviour by individuals. However, in countries with systemic and deeply rooted corruption, corrupt practices may be used by different groups of legal and sometimes illegal actors for illegal objectives. For example, the buying and selling of positions in hospital administration may be part of a clientelistic political party system. Health providers may be fake companies set up for money laundering and other illicit purposes; cartels of doctors or other health professionals may capture specific high-cost treatments to extract rents from health systems; hospital inputs and other equipment may be stolen by small local cartels; and pharmaceutical companies may capture groups of patients or patient organisations for illicit purposes. When designing mitigation strategies, it is important to understand the dynamics of and incentives for individual and group behaviour in order to identify potential allies and opponents of change.
Social, political, and cultural differences in what is considered acceptable or unacceptable behaviour require context-specific understanding. Certain types of conduct universally constitute criminal behaviour or administrative misdemeanour, such as bribes or kickback schemes in procurement, buying and selling of positions, or intentional overbilling. But lines are often blurred. At the service delivery level, informal payments that are seen as socially acceptable gifts and favours in one context may be regarded as unacceptable bribery in another.
It should be recognised that not all forms of unethical behaviour are illegal. While most people might agree that it is wrong for a public physician to have an ownership stake in private medical ancillary services, some countries tightly regulate this conflict of interest while others do not. At the same time, not all practices that are illegal are necessarily seen as illegitimate. Some countries have prohibited certain promotional incentives by the pharmaceutical industry to medical staff, yet there may be fairly broad social acceptance of such practices.
In sum, context matters. An understanding of how corruption manifests itself in a particular national health system, along with an assessment of its prevalence and impact on system performance and health outcomes, is a crucial precondition for the design of mitigation strategies. (Table 2 below provides an overview of key corruption risks in the main health system functions, as well as potential mitigation strategies.)
What are the main tools used to diagnose corruption in health?
An array of tools and initiatives have become available for diagnosis of corruption in the health sector. These help define the problem and generate buy-in for anti-corruption measures; they also help practitioners and policy makers agree on goals and targets and monitor improvement (or deterioration) over time. Some assessment tools focus specifically on experiences or perceptions of corruption and on sectoral risks, while others look more broadly at how the health sector is governed. Some focus on specific areas or sub-sectors within health, such as drugs or human resources. Also, some general international surveys of corruption include assessments of the health sector. Table 1 gives an overview of the main tools available.
However, most of the commonly used tools do not assess high-level corruption in the health sector, that is, at the level of ministers, other high-ranking health authorities at national and subnational levels, or hospital managers. This gap, both in practice and in the literature, needs to be addressed if corruption in health systems is to be tackled seriously and strategically.
Table 1: Selection of tools to identify and measure corruption risks and corruption in the health sector
|
Area |
Issue |
Tool |
|
Corruption perceptions and experiences |
Perceptions of corruption |
|
|
Experiences of corruption |
|
|
|
General |
Sector-wide and cross-cutting issues |
|
|
Pharmaceuticals |
Drug and health product supply chains |
|
|
Individual providers |
Job purchasing |
|
|
Health worker absenteeism |
|
|
|
Informal payments |
Informal payments |
|
|
Budget and resource management |
Budget processes |
|
|
Payroll leakages |
|
|
|
In-kind leakages |
|
Source: Adapted and expanded from Lewis and Pettersson (2009).
How is corruption diagnosed in the health sector in practice?
Given that the forms and dynamics of corruption are highly context-specific, and considering that available assessments of corruption perceptions, experiences, and risks tend to be focused on the country as a whole, the corruption assessment methodology is a crucial element of the design of anti-corruption initiatives in the health sector.
Comprehensive corruption assessments on the initiative of the health sector authorities
Generally speaking, a comprehensive corruption assessment of the health sector provides a good basis for identification of strategic priority areas for action. Such an assessment covers perceptions and experiences; corruption risks and their causes, incentives, and consequences; as well as the tolerance levels of different actors towards corruption (see Box 2 for an example of this approach). In some cases further analysis might be needed: for example, if the administration of public hospitals is one of the priority risk areas, it may be necessary to conduct additional analysis on this topic. Corruption risks and practice often vary between different regions of a country as well as between different types of hospitals or private clinics performing public functions.
Box 2: Corruption risks and tolerance in Colombia’s health sector
In Colombia, a comprehensive assessment of health sector corruption and sector integrity strategies was conducted in 2017 under the auspices of the vice minister of health and the director of the superintendency of health. It analysed perceptions, experiences, and risks of corruption; areas of particular opacity; and levels of tolerance of corruption by internal and external stakeholders. The assessment received technical and financial support from an anti-corruption project funded by the European Union (EU), and was carried out by a national university with solid prior experience in the field of health sector governance.
The assessment was conducted in three phases, using complementary diagnostic tools. First, a series of macro-processes related to public health, health insurance, and service delivery were described in detail, identifying relevant norms, actors and their interactions, and resource flows. Through focus group discussions and key informant interviews, the main risk areas for corruption and opacity were identified within each of the macro-processes in order to select priorities for detailed diagnosis.
In the second phase, priority processes (contracting, service delivery, billing, payments and claims processing, as well as collective interventions for public health) were analysed in depth through a perception and experience survey of system users and an institutional survey of service providers and payers. These surveys were complemented by interviews with health sector staff in a selection of cities. In addition, a national survey was conducted on levels of tolerance to corruption in the health sector.
The third phase consisted of developing, through a participatory process, recommendations for concrete mitigating measures, strategies, and policies directed at the different actors (ministry of health and superintendency, public hospitals, insurers, and provincial health departments).
The assessment process ensured ownership by the lead health institutions through a carefully designed process of regular interaction with the vice minister, the superintendent, and lead officials, validating the methodology and seeking feedback on results in the different phases. At the same time, independence was maintained with respect to the final diagnosis and recommendations in order to ensure trust in the legitimacy of the process and outcome. The assessment was accompanied by a communication and awareness-raising strategy. This included academic seminars; 10 information bulletins on the different steps and partial results; and the presentation and discussion of results with the minister, vice ministers, superintendent, and relevant staff, as well as with professional and health industry associations.
Some important lessons were learned. First, this broad and deep process generated a solid diagnosis of the phenomenon of corruption in the Colombian health sector. The results were concerning and something of a surprise, as irregularities and corrupt practices were found to be even more widespread and systemic than initially thought. The process also made it possible to identify concrete action measures targeted at the different players and aimed at transformative change. Second, leadership at the highest level of the health authorities was crucial in ensuring the support of lower-level directors. Third, the role of the university was crucial as well. It provided an interdisciplinary team composed of several university departments as well as students from different disciplines, involved in continuous research on health sector governance, thus going beyond the role of mere consultant. And finally, the role of the EU-funded project in providing ongoing technical advice and political support was considered invaluable by all involved.
Source: Proyecto Anticorrupción y Transparencia de la Unión Europeo para Colombia (ACTUE 2018).
However, such broad assessments are rare. More common are narrowly tailored corruption studies intended to inform the design of mitigation measures aimed at specific risk areas, such as drug supply, or particular types of misconduct, such as informal payments. The following sections briefly describe several diagnostic approaches.
Health sector–specific diagnosis initiated by anti-corruption bodies
Despite recently increasing attention to corruption in national health systems, sector-wide assessments still tend to be driven by the national anti-corruption authority rather than by the ministry of health. This may be because anti-corruption authorities have an institutional mandate to promote integrity across government, based on international guidance in the anti-corruption field, and such initiatives are aligned with their performance measures. Ministries of health, on the other hand, have few incentives to pursue sector-wide approaches, as these require complex political and operational management and are not clearly aligned with sector goals. The Moroccan case in Box 3 illustrates this tension and provides lessons for sector diagnostics.
Box 3: Lessons from the Moroccan anti-corruption strategy for the health sector
The Moroccan Central Authority for Corruption Prevention (ICPC) opted for a sector approach, identifying the health sector as a priority. The ICPC commissioned a private consulting firm to develop a health sector integrity strategy focused at service delivery level. First, public policies, laws, and regulations for corruption prevention were reviewed. Second, corruption risks and experiences were identified in all service and administrative areas of public health institutions. Data were collected in five regions, 3,500 patients were interviewed, and 87 staff members of public hospitals participated in interviews and focus group discussions. This made it possible to define several typologies of corruption. Within these, a total of 87 corruption risks were identified for key players, including hospitals, health centres, clinics, regional centres for blood transfusion, private laboratories, and the central administration of the ministry. Third, the consultancy developed an action plan aimed at mitigating the risks.
The ICPC delivered the results and recommendations for action in 2011 to the Ministry of Health, but ownership of the process by the health authorities seems to have been weak. This resulted in slow initial implementation, among other effects. According to a 2019 interview with one of the ICPC leaders of the process,* the overall approach to the sector strategy was later reviewed with key sector players, and implementation of actions had improved. An analysis of the results achieved in terms of health goals and outcomes would be useful.
Some lessons learned from this experience are as follows: (a) officials at the highest level of key health sector institutions need to assume ownership of the process, ideally at the diagnostic stage; (b) the process needs to be clearly communicated by the top leadership of the health sector to lower-level officials; (c) pilot projects can boost implementation of the overall strategy; and (d) the anti-corruption authority needs to have the explicit backing of the president if leverage over a powerful line ministry is to be achieved.
* The interview was conducted at a meeting convened by WHO, UNDP, and the Global Fund in February 2019 in Geneva to create a Global Network on Anti-Corruption, Transparency and Accountability in Health (GNACTA).
Source: Hussmann and Fink (2013).
For sector-wide assessments in particular, national oversight and accountability institutions can help identify areas vulnerable to corruption and track progress. These include:
- Office of the auditor general (supreme audit institution): annual audit reports and specific investigations provide insights into vulnerable areas and help pinpoint where leakages occur.
- Anti-corruption commission, inspector general’s office, or ethics office: close cooperation in investigating specific allegations and regular analysis of complaints about alleged corrupt or unethical behaviour can help identify risk areas.
- Parliament: regular interaction with the parliamentary complaints commission and parliamentary accounts committee may provide information about specific risk areas.
In seeking their collaboration, however, attention should be paid to the risks of political influence and patronage that often permeate these institutions in countries with systemic corruption.
Pharmaceutical and medical device sub-systems
Assessments in the pharmaceutical and medical devices sub-system have become more common since around 2005. The most widely applied and referenced methodologies are the Good Governance for Medicines (GGM) instrument and the Medicines Transparency Alliance (MeTA) approach (Box 4). The GGM is mainly government-led, with strong support from WHO, and has been applied in some 30 countries. MeTA is a multi-stakeholder initiative between government, civil society, and the private sector, with support from development partners, and has been piloted in at least seven countries.
Box 4: GGM and MeTA in a nutshell
The World Health Organization has developed within the framework of its Good Governance for Medicines (GGM) programme an assessment instrument to identify corruption risks in the pharmaceutical sector. It is based on a diagnostic tool developed in 2002 for the World Bank’s work in the Costa Rica. According to UNDP (2011), it can ‘potentially examine up to eight core functions: medicines registration, licensing and inspection of pharmaceutical establishments, promotion, clinical trials, selection, procurement, and distribution. The end result is a baseline to monitor the country’s progress over time in terms of governance in the pharmaceutical sector (e.g., level of accountability, transparency in the various processes in the pharmaceutical sector).’ The GGM in its original form is particularly useful for integrated public health systems.
The Medicines Transparency Alliance (MeTA) is a multi-stakeholder alliance, initially led by the UK Department for International Development (DFID) and supported by the World Bank and WHO. ‘It examines issues related to drug prices, quality, availability, promotion, transparency and accountability, and multi-stakeholder relationships… MeTA uses a large arsenal of diagnostic tools to gather information. Such tools may include a pharmaceutical sector scan; review of data availability about price, registration and policies on promotion; and a stakeholder mapping. Priority information sought includes the quality and registration status of medicines, availability of medicines; price of medicines; and policies, practices and data on the promotion of medicines. Also investigated is the specific policy context as well as how supply chain operations work, affordability of medicines, access and their rational use.’
Source: UNDP (2011); see also WHO (2018b).
Intuitional-level diagnostics
Another approach to corruption risk assessment focuses on the institutional level. While all health sector institutions are vulnerable to corruption, corruption risk assessments are more often conducted in provider agencies – health centres, hospitals, clinics – and less often in national health regulatory agencies, public health insurers, or provincial health departments, not to mention ministries of health. As these non-provider institutions are also key players in the health system, their assessment would be a useful area of focus for development partners. In low-income countries, institutional corruption risk or accountability assessments are often part of donor-supported programmes. Middle-income countries are more likely to have national norms that require all public sector institutions to conduct such assessments on a regular basis. However, given that such public sector norms are often implemented in a non-participatory, ‘tick-the-box’ way, there is room for donor-supported technical assistance, as illustrated in Box 5.
Box 5: Turning an anti-corruption assessment from a compliance issue into a management tool: The case of Invima in Colombia
The Colombian drug and food authority is the Instituto Nacional de Vigilancia de Medicamentos y Alimentos, known as Invima. It set out to integrate transparency and integrity as a cross-cutting commitment into its institutional mission under new leadership in 2016.
A first step was to turn a legal instrument called the Plan Anticorrupción y Atención al Ciudadano (Anti-corruption and Citizen Service Plan) into a planning instrument that could be used instead of following the traditional ‘tick-the-box’ exercise to comply with a statutory obligation. Under the leadership of the director, focus group discussions allowed staff to break taboos and talk about corruption within the institution. This allowed the officials to identify corruption risks and develop mitigating measures, including an institutional policy of ‘zero tolerance to corruption.’
A second aspect was to approach ‘accountability’ as a permanent two-way dialogue with users and interest groups, including the different industry sectors regulated and overseen by Invima. Yearly public accountability sessions were preceded by consultations to identify perceived strengths and weaknesses (and areas of opacity) of the processes that Invima is in charge of. The entity was recognised for the innovation and openness of its accountability strategy by certain industry representatives, as well as by the Administrative Department of Public Service (Departamento Administrativo de la Función Pública).
A third initiative was the creation of an ‘integrated management system of transparency and integrity.’ The purpose was to place transparency, integrity, and corruption prevention norms for the public sector at the heart of Invima’s mission, going beyond mere compliance with formal obligations. The director entrusted the implementation of this initiative to a ‘seed group’ of managerial staff from different units in order to overcome existing silos and create staff ownership and empowerment. Assisted by external experts, this group identified priority areas for action, building on the results of the corruption risk analysis and combining prevention with detection and sanctions. An internal and external communication strategy linked all efforts with the commitment of Invima leadership to promote cultural change within the organisation. In addition, Invima implemented a pilot project to train its public officials to identify and respond to ethical dilemmas and corrupt practices. Finally, the entity developed a competition that invited all work units and teams across the institution to submit creative performance pieces spotlighting the institution’s values, including transparency, integrity, and honesty.
For the design and implementation of these initiatives, Invima received technical assistance and modest financial support from an EU-funded anti-corruption project that included a focus on sector integrity strategies.
Some key lessons learned are as follows: (a) leadership of the director and support of the management team were essential in promoting institutional cultural change in favour of transparency, integrity, and accountability; (b) the support of national-level entities such as the Administrative Department of Public Service and the Secretariat of Transparency increased the legitimacy of the initiatives; (c) the internal seed group at managerial level, bringing together the areas of planning, internal control, human resources, and communication, proved crucial for the articulation of the different actions; and (d) the ongoing and flexible support of the international cooperation project was essential for the design and successful implementation of the initiatives.
Source: ACTUE, Estrategia de transparencia en el INVIMA.
Assessment of specific corrupt practices in the health sector
Yet another approach is to conduct assessments of specific corrupt and unethical practices when these have been identified as particularly harmful for health service delivery. Examples include informal payments, absenteeism, and corruption in drug procurement. Based on the available literature, these practices have been analysed in a large number of specific country cases. However, the applied assessment tools seem to vary considerably in the definitions and approaches used, given the great context specificity of these practices.d9e313ffcdfd
Combination of perception-based and experience-based assessments
Ideally, corruption perception assessment tools should be complemented by corruption experience assessment tools. The application of such tools in different settings suggests that there may be considerable discrepancies between their respective results in the health sector (Box 6). In addition, it is useful and sometimes essential to use different experience-based tools for health service users and the general public, on the one hand, and health sector employees or experts, on the other (the latter category includes personnel in medical care, human resources and financial administration, management, logistics, etc.). Triangulating the results from these two types of assessments can help establish a realistic diagnosis of system integrity.
Box 6: Contrasting results from perception-based and experience-based corruption diagnosis tools
In 2013 the Transparency International Global Corruption Barometer (GCB) asked more than 114,000 respondents in 107 countries about their experiences and perceptions of corruption. Perceptions of corruption in the health sector tended to be far higher than reported experiences of bribe paying. In Nigeria, for example, 41% of respondents considered the health sector to be corrupt, but only 9% reported having paid a bribe. In Indonesia this ratio was 47% to 12%. There may be multiple reasons for this gap, but it is clear that people who have had not personally experienced corruption nonetheless may consider parts of or the whole health system to be corrupt, perhaps due to scandals in the media, hearsay, or inefficiencies they have experienced.
Colombia, meanwhile, provides interesting insights into the need to distinguish even between different types of experience. According to the GCB 2013, 62% of Colombian respondents considered the health sector as corrupt, but only 7% reported a personal experience with bribe paying. This led policy makers and experts to believe that corruption levels in Colombia were highly overestimated. However, an in-depth sector corruption assessment by civil society organisations in 2017 found that 55% of the respondents considered the health sector as corrupt, and 53% had witnessed corruption during the past two years. One of the main differences in the 2017 Colombian study was that people were asked about their experience not only with bribes, but also with other forms of corruption like favouritism, influence trafficking, conflicts of interest, and fraud. Experience with bribery stood at 12%, very close to the results of the GCB. This suggests that it is important to conduct in-depth national analysis of perceptions and experiences with a range of common corrupt practices.
Sources: Transparency International Global Corruption Barometer 2013; GES and ACTUE Colombia (2018).
The review of how corruption diagnosis is carried out in practice shows that in many cases a combination of different tools will be useful. This is not an argument for duplication of efforts, but for deciding on an appropriate combination of tools for each context and purpose.
And finally, two important points for development partners. First, donor funding and technical support is essential for health sector corruption assessments. Even in middle-income countries, where the highest level of government may be vested in health sector anti-corruption assessments, it may be impossible to fund the assessments through the cumbersome national budget processes.
Second, promising initial results emerge from three-actor alliances between (a) high-level authorities of health sector institutions, which give strategic direction for assessments that respond to their needs and priorities; (b) development partners, which provide funding as well as technical assistance; and (c) national universities, which conduct the corruption assessments with multi-disciplinary teams involving large numbers of students. Political will at the highest level is an indispensable precondition, albeit not frequently found. At the same time, the involvement of universities helps ensure continuity when public leaders change.
Design of mitigation strategies
Corruption is a public health issue that will not disappear by itself, nor can it be ignored. Donor agencies, international organisations, and national governments have come to explicitly acknowledge the problem. The experience of mitigation strategies in the health sector as well as lessons learned from other sectors will help health advisors of donor agencies, their government counterparts in-country, and other actors recognise that it is possible to confront corruption. Towards that end, this section briefly outlines key elements to be taken into consideration when designing mitigation strategies.
Understanding the enablers and drivers of corruption
A first step is to understand the circumstances that are conducive to corruption. Figure 2 presents a conceptual framework that can be summarised as follows: People are more likely to cross the line between honest and corrupt behaviour when they have an opportunity to misuse their power (in part because the probability of consequences is low); when they feel pressured or incentivised to do so; and when personal or social beliefs and norms allow them to rationalise corrupt behaviour.
Figure 2: Key elements for the design of mitigation strategies
Source: Vian (2008).
Looking more closely at the elements of opportunity included in Figure 2, we see that corrupt behaviour is more likely in situations where some or all of the following conditions are present:
- The agent with entrusted authority has monopoly powers. The agent might be the only provider of health services, medical treatment, or medicines and supplies.
- Officials have discretion without adequate control of their decision-making authority. Such decisions might concern the definition of treatments and drugs to be covered by health insurance, or the prescription of particular medicines, diagnostic tests, or treatments. Discretion is a complex issue due to the tension between control and medical autonomy.
- There is not enough accountability for decisions and actions. Accountability comes through measurement of results and sanctions for non-performance.
- Citizen voice and participation are insufficient to allow for social control – for example, by generating experience-based data on absenteeism, monitoring drug procurement or hospital construction, or exposing undue influence in regulatory and policy decisions.
- Transparency is lacking, in the form of active disclosure of and access to information. This affects, for example, the regulation of market access of drugs and medical devices, the prices of medicines, or prescription behaviour.
- Enforcement is weak. Abuse or corruption is not detected and punishedthrough administrative, fiscal, or penal enforcement or through social sanctions.
Pressures and incentives to engage in corruption can be political, financial, bureaucratic, or social. For example, public officials may feel an obligation to return political favours to superiors, the party, or suppliers. They may feel pressured financially because of low public sector wages. Public officials also may feel social pressure, for example to favour relatives in awarding contracts or filling positions.
Individual beliefs, attitudes, and social value systems influence the likelihood of corruption by allowing those engaged in corrupt practices to rationalise or justify their behaviour. In post-communist Europe and Central Asia, for example, the introduction of capitalism came with the notion that ‘everything has its price.’ In some African societies – indeed, in a range of societies around the world – corruption may be justified by the social imperatives of gift giving, family or ethnic solidarity, or redistributive accumulation.
Key elements of mitigation strategies
An understanding of the circumstances favouring corruption provides a basis for the design of mitigation strategies. The medical and governance fields share a fundamental principle: prevention is better than cure. In line with this, efforts to tackle corruption need to translate the main principles of good governance – information, transparency, integrity, accountability, and participation – into action. High-level political will and leadership is essential.
Efforts to address corruption risks should contain a combination of legal, institutional, and management measures. The linkages between prevention and enforcement require special attention. Of particular relevance, as reflected in Figure 3, are sound management systems and practices that reflect the principles of transparency, accountability, and participation in external oversight. In addition, credible control systems and enforceable sanctions, including audits, internal and external complaints-handling mechanisms,20181fed9ecb and whistle-blower protection, are needed to catch misconduct that could not be prevented. However, in countries with weak rule of law, expectations about the effectiveness of detection and deterrence need to be realistic.
A key challenge is to ensure the appropriate mix and sequencing of these approaches. No single measure alone will bring about real change. For example, active disclosure and free access to information (transparency) about drug-prescribing behaviours needs to be linked to monitoring of the desired result, whether this is to lower costs, reduce unnecessary treatments, or ensure that generic drugs are used where applicable. Monitoring in turn should be linked to reporting of the results (accountability). Finally, detection of improper practice could be facilitated through information systems that feed into the respective oversight institutions (enforcement). In other words, the different elements are mutually reinforcing and need to be combined for transformative change.
Figure 3: Interplay of awareness, prevention, detection, and sanctions in corruption mitigation strategies
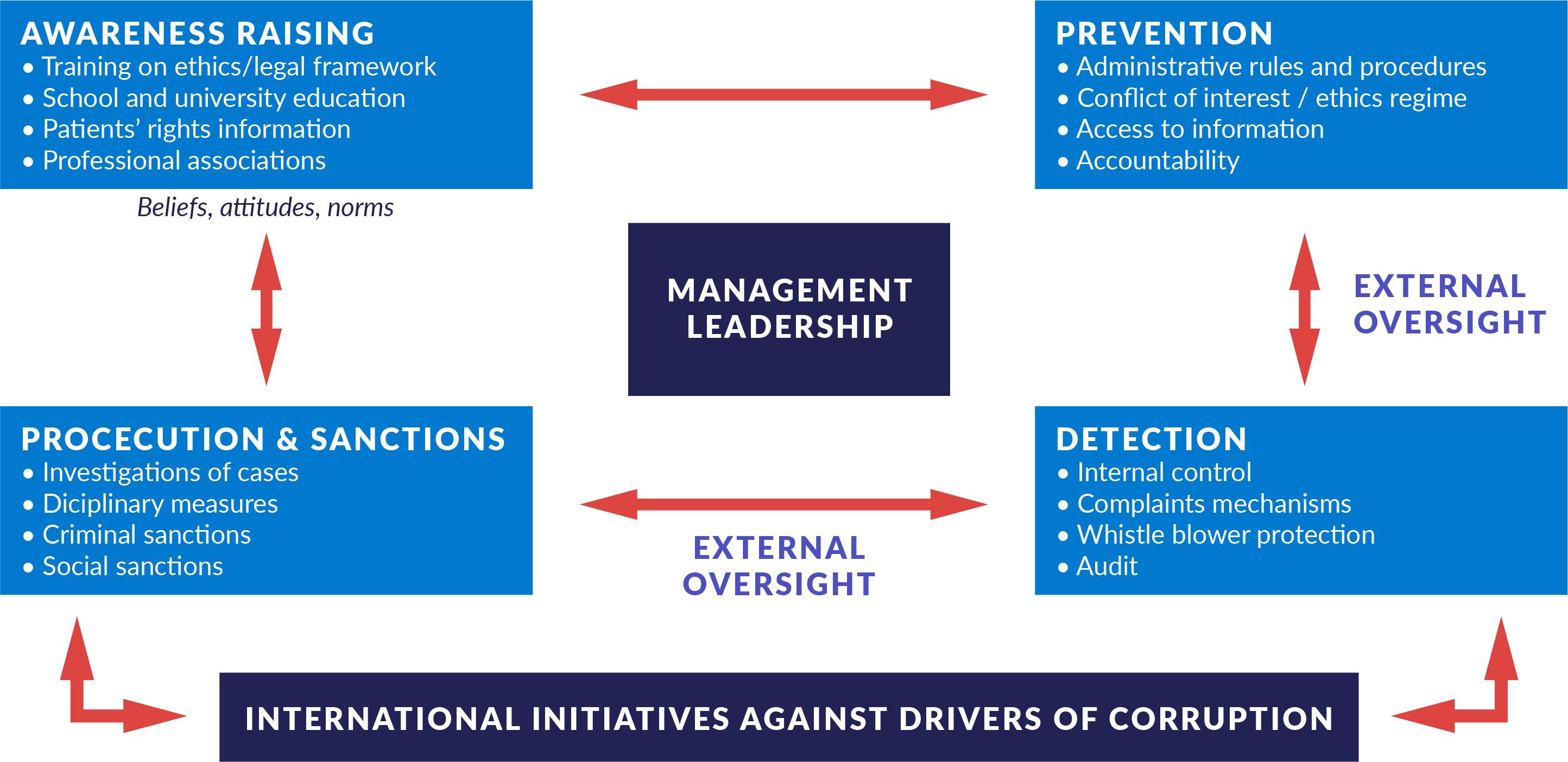
Source: Author.
Corruption prevention and control requires authentic political commitment, high-level leadership, sufficient knowledge of the health sector, and resources to implement the chosen strategies and interventions.25ea4f7391f7 This may sound obvious, but these elements are often lacking in practice due to the political cycles of governments, the programme cycles of development projects, or a combination of both. While political leadership at the highest levels is usually essential to address the most pernicious forms of corruption in the health sector, the lack of such leadership should not be used to justify inaction on the part of donor agencies. Rather, donors should proactively and strategically look for areas, entry points, and/or partners that can promote even incremental change in corruption control while focusing on improving health outcomes.
Finally, the design of anti-corruption interventions should also look at levers that can have an impact on grand corruption in the health sector – for example, national officials channelling large amounts of money from the health budget to bank accounts abroad or to the purchase of property and luxury goods. The undue influence of the international pharmaceutical industry on national drug policy, a form of state capture, also falls in the category of grand corruption. Mitigation measures could include monitoring of the assets, interests, and lifestyles of senior health sector officials as well as scrutiny of their acquisitions and movement of assets, both in-country and internationally. On the development partner side, a whole-of-government approach to corruption in the health sector might be useful.
How has corruption been addressed in the health sector so far?
Corruption in the health sector is increasingly recognised by national governments and civil society in countries around the world; by different health-related industries, in particular the pharmaceutical and medical device industry; as well as by development partners and international organisations. The past decade has seen:
- A growing body of literature on corruption in the health care sector. Since the year 2000, the number of articles has more than doubled.65eb64fa4342
- A growing volume of sector and sub-sector policy, programme, and diagnostic guidance produced by donors and international organisations, including U4, UNDP, WHO, OECD, the World Bank, and DFID, among others.
- The crafting of specific national programmes or strategies to address corruption in the health sector, often supported by development partners.
- The implementation of practice-oriented research initiatives conducted by universities and think tanks from the Global North in partnership with local actors in the Global South, again mostly supported by international development funding.
- Initial steps to create a Global Network on Anti-corruption, Transparency and Accountability in Health, convened jointly by WHO, UNDP and the Global Fund in early 2019.
Countries around the world have made efforts to address corruption and unethical behaviour in health systems. In many if not most cases, the initiatives seem to be targeted at either specific problems (such as informal payments, absenteeism, or overbilling), specific processes (such as drug procurement or health workforce management), or specific institutions (such as health centres, hospitals, and maternity homes). These interventions are often deployed in limited geographic areas, and for limited periods of time. Moreover, the initiatives often seem to be developed in an opportunistic and not necessarily strategic way. Opportunities or imperatives for action may arise, for example, when donor funds become available to support anti-corruption projects in the health sector, or to mainstream a corruption risk approach into health sector programmes; when a government needs to respond to a publicised corruption scandal; or when civil society advocacy pushes the government into action. More holistic, strategic, and medium- to long-term initiatives to address corruption in health systems seem to be rare as yet.
To date, there is little documented evidence on what works and what does not, under what conditions, and with what kinds of results.8093b4e2029d The available literature mainly provides context-specific case studies on issues such as absenteeism, informal payments, theft and embezzlement of drugs and supplies, unnecessary or false procedures, and fraudulent reimbursement claims. There is also a fairly significant body of literature on how to address corruption in the pharmaceutical supply chain. A number of shared methodologies for this have been developed at international level and implemented at country level, with a review of results again from the international perspective.
It should be noted, though, that these considerations derive mainly from literature that is internationally available, mostly in English; a considerable part of it was developed with donor support, either through commissioned or funded research or through project reviews and evaluations. This may result in a distorted picture of the situation. There has been a growing demand for more research and critically documented evidence generated by practitioners and academia.
Table 2 outlines the main types of corruption in the health sector and lists some selected mitigation strategies. For further information on these forms of corruption and mitigation strategies, see Annex 1.
Table 2: Mitigation strategies for different types of corruption risks in health systems
|
Area |
Issue or process |
Type of corruption |
Selected mitigation strategies |
|
Regulation |
Health policy |
|
|
|
Health care financing |
|
||
|
Quality of products, services, facilities, and professionals |
|
||
|
Budget and resource management |
Budget process |
|
|
|
Billing for services |
|
|
|
|
Payroll management |
|
|
|
|
User fee revenue |
|
|
|
|
Use of resources |
|
|
|
|
Procurement |
Construction and rehabilitation of health facilities |
|
|
|
Equipment and supplies |
|
||
|
Drug management |
Approval |
|
|
|
Procurement |
|
||
|
Distribution |
|
||
|
Human resources management |
Appointments and promotions |
|
|
|
Accreditation of health professionals |
|
|
|
|
Time management |
|
|
|
|
Education and training |
|
|
|
|
Service delivery |
Service delivery at facility level |
|
|
Source: Author, with inputs from Vian (2008).
In a number of countries, anti-corruption, transparency, or accountability strategies have been developed for the health sector as a whole. The distinct feature here is that the whole sector was scanned for corruption risks, and on the basis of the results, priority areas for action were selected. This selection does not necessarily address all forms of corruption detected, or even the most harmful forms, as this may be politically or technically infeasible in the short term. Rather, priority might be given to corruption in service delivery, for example, as the area that citizens tend to care most about. However, if well-known forms of high-level corruption are not addressed, the credibility and legitimacy of the strategy might suffer (as was the case in the initial phase of the Moroccan health sector anti-corruption strategy described in Box 3).
In many cases such broad-based sector strategies seem to be supported, and sometimes promoted, by development partners. In cases where the main country counterpart is not the ministry of health but the national anti-corruption agency, special effort is required to achieve full buy-in at ministerial level. Unfortunately, documentation is scarce on the implementation and results of health sector strategies, and on lessons learned – without doubt an important area for comparative research.
A number of international initiatives have been created for the pharmaceutical sub-sector. The Good Governance for Medicines programme and the Medicines Transparency Alliance provide risk assessment methodologies and action plans that have been implemented over several years in the participating countries. Box 7 summarises some lessons learned.
Box 7: Results and lessons learned from MeTA and GGM
A study on MeTA from 2017 found: ‘Countries used evidence gathering, open meetings, and proactive information dissemination to increase transparency. MeTA fostered policy dialogue to bring together the many government, civil society and private company stakeholders concerned with access issues, and provided them with information to understand barriers to access at policy, organisational, and community levels. We found strong evidence that transparency was enhanced. Some evidence suggests that MeTA efforts contributed to new policies and civil society capacity strengthening although the impact on government accountability is not clear.’ The study highlights the importance of involving civil society in monitoring and advocacy for accountability efforts. It further underlines the need for sustained efforts if transparency is to increase accountability of government and other actors in the pharmaceutical sector.
Reviews on the GGM programme found that it increased awareness of transparency and governance in the pharmaceutical sector and contributed to the publication of previously unavailable information. However, it is not clear whether and to what extent corruption may have been controlled. GGM’s effort to actively promote leadership by the ministries of health was noted as important, although the vulnerability to changes in government and to lack of support or involvement from other relevant sub-sector actors, including ministries of finance, was also underlined. In this programme, too, the inclusion of civil society and the private sector was considered relevant.
Sources: Vian et al. (2017); Kohler and Ovtcharenko 2013.
Two global initiatives that aim to promote transparency, accountability, and civil society participation broadly at the state or government level have helped facilitate anti-corruption approaches in the health sector. The Open Government Partnership (OGP) is a multi-stakeholder initiative with close to 80 participating countries. By 2019, a quarter of the members had implemented commitments related to the health sector, including public monitoring of performance, budget and expenditure tracking, policies to address conflicts of interest, and social accountability in health. The OGP notes that ‘health commitments are often more ambitious than commitments in other sectors, but are less successful in significantly improving government openness.’ It calls on participating governments to ‘put citizens in the center of health policy development.’287ee5d234ad An initiative dealing specifically with procurement, the Open Contracting Partnership, works with governments, businesses, civil society organisations, academia, and the media to open up government procurement and address problems such as corruption and lack of transparency. Focusing on the health sector is a potential approach to be pursued.
Corruption in health procurement can lead not only to great financial losses but to drug shortages, inflated prices, and counterfeit medicines. Accordingly, a new initiative was started following the Anti-Corruption Summit in London in 2016, where a number of countries including Argentina, Malta, Mexico, and Nigeria pledged to introduce open contracting into their health sectors. Also, with funding from DFID, the Transparency International Health Initiative is working on a project called Open Contracting for Health (OC4H), with an initial focus on five countries in Asia and Africa.
Specific risk areas of the health sector have recently received attention in terms of policy guidance. The issue of transparency in drug pricing has become an important point on health policy agendas, both national and international. In many countries the cost of medicines accounts for a large proportion of health spending. Moreover, drug prices vary greatly between countries, with some poorer countries paying 10 times the reference price of the same drug in Europe or North America. Efforts to regulate drug prices can generate results, but one of the main challenges is the opacity of drug markets and regulations. Against this backdrop, the World Health Assembly in 2019 approved a milestone resolution on ‘improving the transparency of markets for medicines, vaccines, and other health products.’201e96ce5a68
Clinical trials have been identified as vulnerable to opacity, with severe consequences for the health sector. According to Transparency International UK, ‘This lack of transparency in clinical trials can increase the risk for undue influence, manipulation of data and evidence distortion. It is a symptom of limited regulatory authority over the reporting process. It opens the door to fraud and corruption and undermines both medical advances and public health objectives.’ With civil society partners, TI has developed a practical guide for policy makers on how to foster transparency in this area.9f6158ecaed7
Several countries have experimented with using social accountability measures to curb health sector corruption. A recent study of a programme focusing on maternal health in the Indian state of Uttar Pradesh found that informing women of their rights and teaching them how to lodge complaints yielded substantial results. The initiative reduced bribe taking and informal payments for health services that should have been provided free of charge.0933b2a933ef
Similarly, a 2009 randomised controlled trial and 2012 follow-up research in Uganda revealed that social accountability interventions improved both health service delivery and health outcomes. The interventions facilitated monitoring-oriented citizen engagement with health facility personnel and provided information for citizens about the facilities’ operations. The interventions led to a reduction in mortality of 33% for children under five years old, as well as a 15% reduction in medicines going missing from the facilities and a 13% reduction in staff absenteeism. The 2012 follow-up, which sought to determine the long-term effects of the initial intervention, found that there was still a 23% reduction in under-five child mortality and 27% for children under two, as well as a 12% reduction in medicines going missing.a2818c5065ff
A similar study looked at the impact of community scorecards on reproductive health outcomes in Malawi. Compared to control areas, areas using the scorecards showed significantly greater proportions of women receiving a home visit during pregnancy and a postnatal visit, as well as higher levels of service satisfaction. The scorecards apparently helped facilitate relationships between community members, health service providers, and local government officials by building mutual accountability and promoting locally relevant and feasible solutions to problems.deabba7d6815
Weaving health and governance commitments together: Universal health coverage and the Sustainable Development Goals
As part of the international development agenda, all UN Member States have committed to achieve universal health coverage as part of the Sustainable Development Goals (SDGs) by 2030. According to the World Health Organization, at least half of the world’s population still does not have full coverage of essential services, and around 100 million people are being pushed into extreme poverty because they have to pay for health care.c5a0d7627a7c
According to WHO, universal health coverage means that ‘all individuals and communities receive the health services they need without suffering financial hardship. It includes the full spectrum of essential, quality health services.’db746d07e1cc In addition to improving people’s health, attaining UHC is also expected to help achieve other health-related SDG targets such as those on health outcomes (e.g., mortality, infectious diseases), as well as SDG goals on education and poverty.
Making progress towards UHC requires health system strengthening at country level, as well as efforts to address a number of international health issues such as the pharmaceutical value chain and drug pricing. Critical elements include robust financing structures and the pooling of funds (health insurance); a health workforce with good capacity; good governance of the health sector; sound systems for procurement and supply of medicines and health technologies; and well-functioning health information systems.
All of these elements for the achievement of UHC, however, can be vulnerable to different types of corruption, opacity, and unethical behaviour. In many developing countries corruption affects not only frontline service delivery for UHC, but also the provision and management of the required funding and appropriate regulation. In this sense, corruption should be widely recognised as a severe threat to UHC.
While recognising that each country is unique and can choose its own focus areas for measuring progress towards UHC, WHO also calls for a global approach that allows for comparisons between countries. It suggests that measurement should focus on (a) the proportion of a population that can access essential quality health services, and (b) the proportion of the population that spends a large percentage of their household income on health. Both of these indicators can and should be linked to an approach that assesses the extent to which corruption influences the results.
Three of the Sustainable Development Goals contain commitments relevant to addressing health sector corruption. They include SDG 3, ‘Ensure healthy lives and promote well-being for all at all ages’; SDG 16, ‘Build effective, accountable and inclusive institutions at all levels,’ which includes fighting corruption; and SDG 17, ‘Revitalize the global partnership for sustainable development.’
In each of these SDGs, specific targets and indicators are particularly relevant to health sector corruption. In SDG 3, the most relevant targets are 3.8, achieve universal health coverage, including financial protection and access to quality care; 3.c, increase health financing and retention of the health workforce; and 3.d, strengthen the capacity of countries to manage health risks.
In SDG 16, the most relevant are targets 16.4, reduce illicit financial flows and return stolen assets; 16.5, substantially reduce corruption and bribery in all their forms; 16.6, develop effective, accountable, and transparent institutions; 16.7, ensure responsive, inclusive, and participatory decision-making; and 16.10, ensure public access to information.
For SDG 17, relevant targets include 17.9, enhance international support for targeted capacity building; 17.14, enhance policy coherence for sustainable development; 17.16, enhance multi-stakeholder partnerships to achieve the SDGs; and 17.17, promote public, public-private, and civil society partnerships.
A recent study provides concrete proposals on how these three SDGs could be woven together in order to address corruption in health systems.bece5014fecc The study first presents examples of how different types corruption affect the SDG 3 targets and indicators, and then suggests how SDG 16 and SDG 17 targets and indicators could be applied in relation to health sector corruption (see Table 3).
Table 3: Non-health SDGs with potential application to health sector corruption
|
SDG goal and target |
SDG indicators |
Implications for health sector corruption |
|
16.5: Substantially reduce corruption and bribery in all their forms |
16.5.1 and 16.5.2: Proportion of persons or businesses who had at least one contact with a public official and who paid a bribe or were asked to bribe during the previous 12 months |
Could be used to measure how many people have paid a bribe in the public health sector |
|
16.6: Develop effective, accountable and transparent institutions at all levels |
16.6.1: Primary government expenditures as a proportion of original approved budget, by sector 16.6.2: Proportion of the population satisfied with their last experience of public services |
Could be used to measure misallocation of health sector funds |
|
17.14: Enhance policy coherence for sustainable development |
17.14.1: Number of countries with mechanisms in place to enhance policy coherence of sustainable development |
Need to establish policy coherence around international and regional laws, regulations, and enforcement against health-related corruption |
|
17.16: Enhance the global partnership for sustainable development, complemented by multi-stakeholder partnerships that mobilise and share knowledge, expertise, technology and financial resources, to support the achievement of the SDGs in all countries, in particular developing countries |
17.16.1: Number of countries reporting progress in multi-stakeholder development effectiveness monitoring frameworks that support the achievement of the SDGs |
Need to establish multi-stakeholder partnerships that monitor progress towards these goals specifically in the health sector |
Source: Mackey, Vian, and Kohler (2018).
The authors of the study suggest that the UN’s Inter-agency and Expert Group on SDG Indicators should work with WHO on creating a multi-stakeholder partnership to strengthen coherence in programming and policies relevant to addressing the ‘disease of corruption.’
Reflections on the approaches pursued so far
Given that corruption is an important barrier to health access and has a serious impact on health outcomes (see section 1), the framing of anti-corruption and transparency approaches needs to be more clearly linked with health outcomes and with the policy goals of the health sector. Reducing corruption and promoting good governance should not be seen as ends in themselves, but as a means to achieve sector goals. Such an approach could generate support from different actors in the system even for unpopular measures. Most importantly, it could be politically attractive to the senior health leadership, as their performance would be assessed in view of health sector outcomes and not in terms of curbing corruption per se.
There has been considerable progress in diagnosing and understanding corruption in the health sector, as well as in the design of methodologies for this purpose. Although each country context requires its own specific analysis, the available literature and policy guidance (on systems or sub-systems, as well as on specific phenomena like absenteeism, informal payments, drug procurement, or clinical trials) allows interested actors to build a sufficiently strong narrative to promote specific anti-corruption initiatives in a given country. Also, the available diagnostic tools provide a pool of references to draw from in designing a purpose-tailored set of instruments (see Box 2 for an example).
However, there is often a significant gap between the identification of problems, the strategic design of interventions to address problems, and the implementation of these measures. The tools used are often normative and prescriptive, focusing on rules and procedures that are assumed to prevent corrupt practices, but these tools may not adequately capture the complex dynamics that lead to a specific corrupt behaviour. Also, there is a tendency to underestimate the financial and especially the human resources that will be needed over time to implement, monitor, adapt where necessary, evaluate, and communicate the results of the measures undertaken.
The design and implementation tend to be documented in context-specific cases studies, often focused on corrupt practices at the service delivery level. Given that there is no one-size-fits-all approach, there is a need for forums in which experts and other stakeholders can exchange experiences and best practices. Towards this end, steps should be taken to strengthen existing knowledge hubs and centres of excellence and develop new ones.
Documented evidence on outcomes of the initiatives is patchy at the best, and even less is known about impact.27d152b5baca Sometimes evaluations or studies are conducted on particular tools and their effectiveness in improving health sector governance, but without making a clear link to processes or outcomes in the health sector. High-quality studies, comparative where possible, are needed to assess the effects of anti-corruption strategies, with a special focus on their links to health sector goals and outcomes.
There is a surprising lack of documented evidence on initiatives to analyse and address policy, regulatory, and institutional capture in health. Particularly rare are initiatives to strengthen the integrity of health regulatory agencies (such as the US Food and Drug Administration), specific health sector oversight agencies (like the superintendencies in some Latin American countries), health technology assessment agencies, drug price commissions, and national drug procurement and distribution agencies – all entities that play a large role in the health system.
It would be useful to build on the lessons learned from multi-stakeholder health sector initiatives such as MeTA and GGM, as well as from similar approaches in other sectors, to create new such initiatives or develop new versions of those mentioned.8b37037de3da Multi-stakeholder initiatives, typically involving government, civil society, the private sector, academia, and professional organisations, are challenging to implement, but they have the potential to incubate and sustain change through the collective negotiation and monitoring of sector-relevant commitments of transparency and accountability.
A significant amount of aid to the health sector is channelled through multi-donor trust funds.b17767705db6 Efforts to address corruption in such funds may be complicated by a lack of shared understanding – among the funding partners, fund administrator/trustee, implementation partners, national authorities, and intended beneficiaries – as to what constitutes corruption. Accordingly, the donor community should streamline their approaches in this realm. Ongoing efforts to harmonise anti-corruption approaches by the various multi-partner funds are welcome, as funding requirements have been found to foster bureaucratisation by creating new governance structures and processes for accessing funding in the already overstretched health bureaucracies of recipient countries.d960c75cbc74
Private sector engagement in anti-corruption and pro-integrity initiatives in the health sector has not received the required attention as yet at either the international or national level. At the international level, most major pharmaceutical companies, for example, score low on the Access to Medicine Index, indicating a lack of engagement with the access issues that facilitate corrupt practices. In its most recent report, the Access to Medicine Index found that only one-quarter of pharmaceutical companies had banned political financial contributions. At the national level, the pharma and medical supply sector, in particular, may engage in self-regulatory initiatives related to codes of ethics and/or compliance programmes, but these often lack independent and effective complaint and monitoring mechanisms. More should be done to promote initiatives with professional associations of medical doctors and other providers and associations that represent private insurance companies.
Social accountability tools show promise for reducing corruption in health service delivery. However, we need more studies and meta-evaluations of past and ongoing initiatives to understand better the conditions under which social accountability works and does not work. The current country examples we have, while exciting, are difficult to generalise.
Despite the direct effect of health sector corruption on people’s lives, the vast amounts of money spent on health, and the global character of the multi-billion-dollar pharma and medical supply industry, global discussions on anti-corruption initiatives tend to pay scant attention to corruption in the health sector. This is something that must change in the near future if reform is to gain traction.
What can donors do to support anti-corruption, transparency, and integrity in the health sector?
It is time for donors to deepen their commitment to address an issue that has been, for a long time, considered taboo or too complex to be addressed.ac71b6f806ac As this U4 Issue shows, there have been more and more explicit efforts to tackle corruption in health systems, lifting the veil of secrecy to some extent. But there is still a long a way to go to address corruption in health systems openly and effectively. It is crucial to develop long-term, strategic approaches based on a sound understanding of dynamics in the sector and the roles of the different actors, with broad participation by government, oversight institutions, civil society, academia, and the private sector. Donors can play an essential and strategic role in this mix.
International level
Establish linkages and synergies between the SDGs on health, on strong and transparent institutions, and on multi-stakeholder approaches (SDGs 3, 16, and 17)
Donors can use the Sustainable Development Goals to promote a more coherent and systematic approach to anti-corruption, transparency, and accountability in health systems from an international perspective. The SDGs are crucial to the development of national goals and policies, to reporting on progress towards these goals to both national and international stakeholders, and to the allocation of funds, in particular from the international community. As noted above, the linking of SDG 3 (promote healthy lives) with SDG 16 (fight corruption and build transparent and accountable institutions) and SDG 17 (strengthen multi-stakeholder approaches for more effective policy making) can provide an important avenue for engagement by development partners.
Towards this end, donors could call on the UN and its specialised agencies, in particular WHO, to develop a practical approach for using the SDG commitments to measure and address corruption in health systems at country level.769dbc14a116 Donors could also pilot the development of such an approach from the bottom up in selected countries. Ideally this would be done in different types of health systems, with different degrees of institutional maturity, in order to explore and test the type of information needed at country level. Valuable lessons learned could be fed into the development of international guidance on this matter.
Support multi-stakeholder initiatives, both health-specific and general, to address corruption in health
Multi-stakeholder initiatives (MSI) have been used to address complex corruption issues in different sectors, including extractive industries, construction, and contracting, among others. MSIs are certainly no panacea; their efficacy and legitimacy tend to be fragile, and they can be misused for image whitewashing. They can, nonetheless, provide a platform for policy dialogue and for commitments to transformative change.
With respect to the drug supply chain, as described earlier, the Good Governance for Medicines instrument and the Medicines Transparency Alliance have generated results and lessons learned. Donors could support the development of new versions of either of them or the creation of a new, potentially merged model. It would be useful to involve some key actors with experience in the MSIs of other sectors in order to build on the strengths of these existing initiatives and try to avoid their pitfalls.
Donors should also proactively use existing MSIs, like the Open Contracting Partnership and Open Government Partnership, to promote a specific focus on health-related corruption, opacity, and accountability. As these initiatives receive important support from donors, this should be quite feasible. Open Contracting could focus on the procurement of drugs and supplies for hospitals, health centres, and ambulances, to name but a few. In fact, Transparency International’s Open Contracting for Health is currently piloting such an approach. OGP action plans are a potential vehicle for efforts to stimulate or strengthen transparency and integrity initiatives in the health sector.146cd22a558b Rigorous monitoring and evaluation of results can help ensure that the commitments are transformative in nature and not just window-dressing.
Finally, donors could consider supporting the creation of one or several international communities of practice around corruption, transparency, and accountability in health systems. The many different areas of health systems tend to involve fairly specialised professionals, institutions, and/or units. While it is important to have a ‘systems’ view to avoid disconnected knowledge silos, an umbrella initiative encompassing all relevant groups might be unmanageable. This tension would need to be resolved over time. An initial step forward is the creation of the Global Network on Anti-corruption, Transparency and Accountability in Health (GNACTA) led by the WHO, UNDP, and the Global Fund as initial drivers.
Broaden support for continuous research and learning on corruption and anti-corruption in health systems
There is a clear need for more documented and critically analysed evidence. This is particularly true in terms of understanding what works, what does not, under what circumstances, and with what results, intended and unintended. Comparative reviews would be especially useful to inform programme design. There is a great need for analysis of how policy, regulatory, and institutional capture plays out in different contexts and of the results of (often still-incipient) mitigation strategies. At the service delivery level, where the lines between unethical behaviour, irregularities, and corrupt practices are often blurred, a good understanding of which forms of behaviour are socially accepted and which are not would provide important inputs for the selection of priority actions. And the list goes on.
Donors should build on and broaden their support for continuous applied policy research and evidence-based policy making. This could include both new research and an inventory of existing research initiatives at the global level, with a searchable database that would host case studies and research documents.47ea658785ab These steps could help policy makers and practitioners learn from success and, importantly, from failure.
In addition, donor agencies could strengthen support for research networks run by universities, organisations, and foundations with a view to generating more documented evidence around anti-corruption and pro-transparency and integrity initiatives in the health sector. Such research should examine successes and failures, intended and unintended results, and facilitating factors and obstacles, with special emphasis on comparative perspectives. Valuable lessons can be learned not just from effective approaches but from erroneous hypotheses and strategies and even outright failures. ‘Open science’ principles should be adopted to ensure that the research is transparent and replicable.
Work with vertical programmes: complement the current fraud control focus with a health systems strengthening approach to increase integrity and accountability in partner systems
Global disease-specific or vertical programmes, such as the Global Fund to Fight AIDS, Tuberculosis and Malaria, the Gavi vaccine alliance, and the President’s Emergency Plan for AIDS Relief (PEPFAR), manage enormous amounts of international donor money, both from bilateral government funding sources and from philanthropic organisations like the Bill & Melinda Gates Foundation. These programmes make great efforts to ensure transparency and accountability in the management of their own funds, focusing specifically on risk management approaches and anti-fraud systems and pursuing a zero-tolerance policy in this regard. However, a narrow focus on fraud prevention runs the risk of ignoring other forms of corruption, such as absenteeism and conflicts of interest, that compromise the health of citizens. Also commonly overlooked is the wider political and economic context, especially the role of patronage, nepotism, and cronyism in facilitating collusion in fraudulent schemes. Vertical programmes do invest to some extent in interventions to strengthen health systems in partner countries, especially the areas of those systems that provide service delivery related to the specific diseases that the global programmes address.
Donor agencies, both bilateral funders and philanthropic foundations, should step up efforts to strengthen health systems in partner countries, placing emphasis on reducing opportunities for corruption. The current fraud control approach should be complemented with country-specific strategies to increase transparency, integrity, and accountability in partner health systems. Ideally, such an approach would be coordinated among the different vertical programmes as well as with other donor-funded programmes that support health system performance in partner countries. For this purpose, each country-level donor coordination group should include at least one governance, transparency, and anti-corruption expert (as distinct from fraud expert). Considering the large amounts of money channelled through the vertical programmes, such an approach could provide an important incentive for action on the ground.
Strengthen civil society initiatives at the international level
Donor agencies could also support civil society organisations to engage in monitoring and advocacy activities at the global level around issues like drug pricing; regulation of market access of new health technologies; private sector compliance with transparency, integrity, and anti-corruption standards (as the Access to Medicine Foundation does, for example); integrity standards and conflict of interest management for health regulatory and oversight institutions; open contracting in the health sector (e.g., as currently done by the Transparency International Health Initiative through a pilot project); and private sector funding and lobbying of international organisations relevant to the health sector such as WHO and the European Medicines Agency, among others.
At the same time, by supporting civil society organisations in multi-stakeholder initiatives, donors can help ensure that civil society is able to participate proactively and offer constructive criticism in partnerships with government (as in the case of OGP) or with government and the private sector (as in the case of a renewed MeTA).
National level
Information and knowledge generation
Support multi-disciplinary diagnostics of corruption, opacity, and tolerance of corruption
Donors with investments in the health sectors of specific countries should consider supporting the development of broad-based diagnostics of corruption, focusing on perceptions, experiences, risks, and tolerance, and using a variety of tools, as discussed above. This could help promote contextual understanding of the phenomenon and its scale and provide evidence-based input for the selection of priorities and design of mitigating measures. Such donor-supported research could be part of an anti-corruption mainstreaming approach for the health sector, or it might be part of a broader anti-corruption programme in the same country.
Donor agencies should ensure close collaboration between their health and anti-corruption teams. Given that such broad-based corruption assessments would benefit all donors, as well as other health sector players, in a country, it could be useful to conduct the research on behalf of or under the auspices of the health sector donor coordination group, if one exists. Ideally, assessments of this type would be realised by respected national universities, in close coordination with but independent of the respective ministry of health and other health sector institutions. National anti-corruption institutions could be invited to accompany the process but should not be the main national counterpart. The results would inform actions by all interested actors, including the donors themselves.
Creation of an evidence base through diagnostics is a particularly relevant area for donor support because governments often face limitations in committing public money for such purposes. Nonetheless, political will at the highest level of a country’s health sector to address corruption is a crucial precondition for success.
Foster external monitoring and oversight
External oversight and monitoring is crucial if anti-corruption, transparency, and accountability measures are to be effective and sustainable. Donors should pay particular attention to two areas:
- Strengthening national health sector oversight institutions, such as health superintendencies or national audit institutions, with a focus on their capacity to identify and act upon irregularities and suspicion of corrupt practices in the health sector; and
- Supporting civil society monitoring and social control of areas in health systems and service delivery that are particularly vulnerable to corruption, opacity, and unethical behaviour (see below for more detail).
Health strategy and policy
Ensure that national development and poverty reduction strategies include corruption diagnostics and mitigation strategies for the health sector
To support sector efforts, performance indicators on corruption in the health sector should be integrated into national development, sustainable development, and poverty reduction strategies and monitoring frameworks.58e2ca2dbb01 High-level donor dialogue and progress monitoring is usually based on the objectives and indicators of these national documents. Accordingly, they can be used to promote political commitment at the highest levels of government to address the most pressing corruption issues in the health sector.
As specific governance and anti-corruption commitments are usually contained in separate chapters of national development or poverty reduction strategies, linkages between the two areas need to be established. This may come more easily if anti-corruption efforts in the health sector are linked with the national anti-corruption strategy. Connecting this with SDGs 3, 16, and 17 may be helpful, as discussed above.
Sceptics may argue that a focus on these high-level policy instruments is unlikely to bring about change, but they offer a valuable opportunity to strengthen ownership and alignment.
Integrate anti-corruption, transparency, and integrity strategies into health policies and plans
The systematic integration of anti-corruption measures into health sector plans and strategies is relatively new, but lessons are emerging. As country contexts vary widely, there is no single blueprint. Health advisors must work closely with governance advisors, with government, and with partners (World Bank, WHO, civil society) to identify the most appropriate approach. Some key elements are set out in Box 8.
Box 8: Key elements for integrating anti-corruption measures into health plans or strategies
- Analyse the nature of corruption in general in the country, taking into consideration local norms and beliefs, legislation, and international standards. Many countries have an anti-corruption law that defines corruption.
- Strive to understand which approaches to addressing corruption in the country have or have not worked so far, including in sectors other than health.
- Identify the types of corrupt practices present in the health sector, and their scope and seriousness, ideally in collaboration with government, partners, and civil society.
- Conduct political economy analysis in the health sector to assess the roles, power, and motivations of individual players. Analyse why corruption occurs, applying principles of governance, economics, and crime prevention to understand the drivers and enabling factors.
- Identify the costs and consequences of corruption and select priorities for interventions. Be realistic and ‘opportunistic’ in choosing priorities, taking the results of political economy analysis into consideration. Aim for visible if modest results that can generate traction and support.
- Design strategies as part of health sector plans and facility governance and management systems. Avoid stand-alone approaches.
- Ensure that the levers of change described in the framework above are appropriately taken into consideration for analysis and design.
- Select a combination of supply-side and demand-side interventions according to the country context and the relative performance and strengths of the different actors. Emphasise civic participation in monitoring services and holding health providers to account.
- Link anti-corruption approaches in health with national anti-corruption policies and foster institutional cooperation between relevant agencies.
- Combine measures to raise awareness of relevant stakeholders; management systems, tools, and practices aimed at prevention; internal and external oversight for detection; and enforceable sanctions to punish and deter abuse.
- Link facility-level efforts with national and international efforts and vice versa.
- Establish baselines and create a sound monitoring and evaluation system to measure results and identify unintended negative consequences. Quantify losses to corruption in health systems where possible.
- Create a communication strategy to frame the issues, advocate for reform, and sustain political and public support, including a clear and simple statement of the problems that need to be addressed. The more challenging the reform process, the greater the need for an effective communication strategy that promotes ownership among key constituencies.
- Identify risks and establish a dynamic risk management system, including at the technical and political levels of the reforms.
- Strive to maintain buy-in on the part of key actors. Even for committed reformers, political reform processes are challenging; this is particularly true of anti-corruption measures, which tend to impact power relations and the distribution of economic resources.
Support the development of transparency or integrity strategies for the health sector
Alternatively, a health sector transparency or integrity strategy can be developed to complement and strengthen existing health sector plans. Such a strategy would assess current levels and risks of corruption; identify constraints and bottlenecks; coordinate dialogue among all stakeholders to select priorities and agree on appropriate, context-specific interventions; and propose ways to implement sustainable change within institutions. The strategy should draw on and feed into national anti-corruption policies in order to ensure coherence with national priorities and make full use of synergies.
Examples of such a strategy can be found in the Colombian and Moroccan cases referred to above, although with distinct approaches and sources of leadership. The transparency strategy for the Colombian health sector was designed on the initiative of the minister, vice minister, and superintendent of health. It builds on the national legal infrastructure and concentrates on policy, regulatory, and institutional strengthening, but with no involvement of the government anti-corruption body, the Transparency Secretariat. On the other hand, the Moroccan health sector anti-corruption strategy was initiated and mainly guided by the country’s anti-corruption authority, with a strong focus on service delivery.
Health advisors should consider a phased implementation approach, focusing on issues that are doable within the comfort zone of government counterparts before attempting more ambitious and difficult tasks. Similarly, advisors should consider conducting pilot initiatives that produce a demonstration effect and can then be scaled up.
Support South-South exchange around health sector integrity initiatives
Peer-to-peer initiatives that aim to strengthen specific policies, regulations, or institutions of the health sector can be promising and at times powerful approaches to achieve difficult reforms and monitor results of implementation. The area of pharmaceutical policy and the drug supply chain, in particular, offers valuable examples in this regard. For example, the EUROsociAL II programme has supported peer-to-peer exchange and learning among various Latin American governments on transparency, access to information, and conflict of interests in certain areas of pharma policy.8a64fd921107
Donors should consider supporting exchange and technical assistance among peer health institutions in the South, in particular at regional level, as part of new or existing programmes. Such an approach might be complemented by technical assistance to help build the capacity for real implementation.
Introduce a focus on corruption and integrity in health into government-donor dialogue
Government-donor dialogue should include sector-wide agreements on priority issues related to corruption in the health sector. A few benchmarks and measurable indicators should be agreed upon and tracked through regular high-level and technical working group meetings. Terminology may matter, and should be carefully analysed.7d6a29c3f98c
Examples of how to put this into practice include the use of UNCAC as a reference framework. The linking of the above-mentioned SDGs on health and good governance could be an alternative or complementary approach. Joint government and partner government sector agreements (e.g., International Health Partnership country compacts, health sector MoUs) can be used to secure information sharing, define accountability requirements, and monitor anti-corruption measures. Such agreements can also set out in advance how donors will respond in case of corruption scandals or deterioration in governance. Evidence is emerging that sustained pressure through collective donor responses, combined with support for reform programmes, has the potential to improve accountability.3387bbea7ef6
Discussions on external audits (both financial and performance) could be included as an agenda item in the annual joint health sector reviews. Annual comparisons of essential drug procurement prices with international drug price lists published by WHO could be conducted, and the analysis of major procurements, using fraud detection software, could identify potential patterns of corruption. Steps should be taken to ensure civil society participation in government-partner dialogue, both in providing evidence-based monitoring of health provider performance and in holding providers to account. Major donors like DFID are well placed to foster a supportive donor response to corruption in health; DFID stands out for its comparative advantages in donor coordination, health sector engagement, and governance.
Targeted reforms and measures
Strengthen regulatory and institutional transparency and integrity
Ill-informed, distorted, and/or captured health policies and regulations have an enormous impact on health sector corruption. Indeed, capture of the state policy and regulatory apparatus by powerful groups can be seen as a primary driver of corruption in the sector. Donors should give high priority to strengthening the transparency and accountability of key policy-making and regulatory processes with a view to managing conflicts of interests. Crucial areas include drug pricing; market access of new drugs and health technologies; clinical trials; accreditation of health providers; definition of benefit packages; independent information on drug use and prices; procurement of drugs and supplies; and laws to promote transparency of relations between the industry and health service providers (‘Sunshine Acts’).c291668c6510
Donors should provide systematic technical and political support to strengthen key health sector regulatory and oversight institutions, as well as the ministries of health, in order to create mechanisms for transparency, integrity, and accountability that function effectively and can gain public trust. The design of such mechanisms should be based on institutional ‘integrity screenings’ developed in a participatory way with internal (and possibly also external) stakeholders.
Donors could support such initiatives in a series of hospitals at different levels of the public administration and in different regions, using control groups in order to assess effectiveness. It may be strategic to focus initially on areas where high-level political and/or technocratic leadership with a strong interest in promoting reform can be identified.
Use opportunities for specific measures
Comprehensive anti-corruption reform requires strong political will and/or specific drivers that tend to be outside the control of development partners. Given these barriers, donors can make strategic use of less ambitious, more finely targeted approaches to address specific corruption problems or risk areas when and where such opportunities arise. This may occur in the wake of a major scandal, or as part of a wider drive to improve value for money and development effectiveness.
These specific interventions and the associated technical assistance may sometimes provide the starting point for other interventions and may even lead over time to a more comprehensive approach. For example, initial support for interventions to address informal payments and absenteeism among certain health providers may result in support for overall institutional integrity strengthening. Or initial support for transparent drug price regulation or procurement could lead to a broader transparency strategy for the pharmaceutical supply chain, as happened in Colombia.
In addition to responding to the particular needs and interests of government counterparts in country, donors should use the above-suggested diagnostic approach, together with a stakeholder or political economy analysis, to identify targeted entry points for donor engagement. This may open the way for more difficult and/or comprehensive reforms at a later stage.
However, anti-corruption measures ideally should not be the result of an ad hoc reaction. Efforts to address corruption tend to generate high expectations on the part of those affected by corruption as well as, at times, strong resistance from those who stand to lose from reform. Both sides need to be managed carefully if the intervention is to be successful and sustainable.
Build bridges between the health and anti-corruption/governance communities
Most countries have just one or perhaps a few central government bodies whose mandate is to prevent corruption and promote good governance, transparency, and integrity. They are tasked with building capacity in this area, overseeing the design and implementation of measures, and monitoring the results. These institutions tend to have a very limited number of staff, in most cases concentrated in the capital city. Yet they are expected to work across the whole of government, providing support, technical assistance, and advice to all sectors at all levels. It comes as no surprise, then, that in most cases the interactions between anti-corruption/transparency bodies and sector institutions, including those in health, are rudimentary, limited to awareness-raising exercises and general guidance delivered in booklets.
For their part, the staff of health sector institutions are educated in the medical professions or in health administration and management. Despite general knowledge of governance and integrity norms for their fields, they may implement these norms from a ‘tick-the-box’ or compliance perspective, at best. Capacity and skills to develop a real management culture of transparency and integrity are often in short supply.
Donor agencies can support technical assistance programmes that build bridges between these two communities. They can help health sector institutions implement existing transparency, integrity, and accountability norms in such a way as to clearly foster their own institutional missions while also linking to a comprehensive institutional integrity management system. At the same time, donors can help the national anti-corruption/transparency bodies develop health sector–specific guidance and capacity building and provide spaces for policy coordination and performance monitoring.
Civil society, academia, and the private sector
Strengthen civil society for social control and advocacy for transparency and integrity
Civil society organisations (CSOs) and other nongovernment actors usually focus either on good governance/anti-corruption issues or on health sector–specific work, but rarely on both. CSOs and professional organisations in the health field tend to concentrate on public health issues and professional ethics. Although they monitor service delivery and may look at specific problems such as informal payments or absenteeism, they usually do not monitor corruption in the sector from a broader governance perspective. On the other hand, CSOs dealing with transparency, accountability, and corruption usually do not work specifically on the health sector, except for some targeted initiatives often related to (drug) procurement.
Donors can help facilitate cross-fertilisation and cooperation between these two types of civil society organisations. Building coalitions between health sector CSOs and anti-corruption/governance CSOs can help create synergies between the two distinct fields of practice and also increase the political weight and voice of the CSOs. For instance, CSOs working on social accountability initiatives in the health sector could receive assistance from anti-corruption CSOs in enforcing accountability through the legal system when monitoring activities uncover corruption. Donors can also support civil society efforts to mobilise policy advocacy and grassroots anti-corruption campaigns focused on health. Financial, technical, and political support to CSOs should be conceived from a medium- to long-term perspective, in part so that CSOs doing anti-corruption work in the health sector can sustain these efforts when there is a change of government.
Pilot national multi-stakeholder initiatives for transparency, integrity, and accountability
Actors who are part of the problem of corruption also need to be part of the solution. Building on the lessons learned from multi-stakeholder initiatives in health and other sectors at global level, donors could support the development and piloting of multi-stakeholder initiatives at national level. They could support government actors, private sector associations, doctors’ associations, independent civil society, academia, and others in collective efforts to jointly develop an understanding of priority corruption and integrity risks in the sector and the key measures needed to address them. A strong monitoring and mutual accountability mechanism should be built into such an initiative. Political will and leadership of health sector authorities in the country is a crucial precondition.
Support integrity and transparency initiatives in professional associations
In most countries, anti-corruption and integrity initiatives in the health sector have focused on the public sector, to a lesser degree on the health technology industry, and at service delivery level on individual medical staff. Largely lacking are transparency and accountability initiatives among professional organisations in the health sector, such as associations of medical doctors and specialists (surgeons, anaesthesiologists, etc.) and health administrators. Such initiatives could be valuable, as professional organisations play key roles in guiding, regulating, and where necessary, disciplining the conduct of doctors and other health professionals.
Donors could support the development and initial implementation of transparency and integrity initiatives by professional associations in the health sector. Some financial resources will be needed to help kick-start the process, but equally important are technical assistance and facilitation for the design and preparation of initiatives, for rigorous results monitoring, and for peer learning around experiences and best practices.
With respect to the pharmaceutical and medical supply industry, self-regulation initiatives dealing with transparency and ethical conduct are key. Donors could support peer-to-peer learning among these industry associations and also support civil society in monitoring their effectiveness. Funds for the development of such initiatives should be raised by the industry associations themselves.
Support national-level teaching and research
The knowledge base on corruption, its different forms in the health sector, and the effectiveness of mitigation strategies is still patchy in many places. One fruitful area for donor support is the funding of national-level research that can provide a basis for policy and regulatory development and for impact monitoring. In many cases government budgets do not allow this type of expenditure, or procedures may be so cumbersome that the research never gets off the ground. Donor support in this area is particularly appreciated and vital.
Actions for development partners themselves
Promote cooperation between health and governance teams/advisors within donor agencies
Every donor agency should promote and incentivise closer cooperation between its health and governance teams, in particular at country level. Health advisors need to work closely with governance advisors to:
- Incorporate a corruption risk and integrity lens into new health programmes, starting from the first discussions and mainstreaming this approach throughout the process.
- Analyse and understand the general context of corruption in the country.
- Support the development of corruption and stakeholder analysis for the health sector.
- Review the specific corruption vulnerabilities in the health sector and support the selection of priorities as well as the design of mitigation strategies.
- Identify ‘red flags’. Health advisors should have the skills to spot and react appropriately to incidents of corruption in the sector.
- Contact the appropriate fraud unit if they suspect or know of any fraud, corrupt practice, theft, or other misuse of agency funds, affecting either direct funding or funds channelled through a third party.
- Build bridges between health sector support and national anti-corruption policies, programmes, and initiatives, as well as with relevant broader governance reform issues.
- Establish linkages with efforts to address grand corruption. Such efforts may include asset declaration and monitoring systems as well as the scrutinising of unusual or suspicious transfers of money by (senior) health officials. Also, ‘due diligence’ checks on senior government officials with whom an agency signs financial agreements may be used.
- Link whole-of-government approaches to the health sector, including support for criminal investigation of corruption allegations against high-level health sector officials, the use of visa denials, freezing of assets in donor home countries, and so on, starting with pilots.
The health sector donor advisory cadre should interact with relevant governance/anti-corruption donor groups for mutual benefit. Advisors can also draw on materials and expertise of the U4 Anti-Corruption Resource Centre.6a97284b31dc
Include anti-corruption and integrity issues in donor coordination on health at country level
In many if not most countries, donor agencies have a health sector coordinating group, sometimes with participation of government partners and sometimes as a distinct space only for donor agencies. This group may discuss broad governance-related issues, and one or another donor agency may support certain corruption prevention or transparency initiatives in the sector. However, it is rare for such groups to integrate a holistic and systematic approach to health sector corruption into country-level donor coordination, and there is great scope for improvement in this regard. In contexts where the government does not have a strong and explicit commitment to work on corruption in its health system, this will not be easy. But in most cases there are ways to address the issue creatively, framing the discussions around transparency and access to information (an area where many countries now have specific laws), integrity, and/or accountability (areas where most countries also have laws or executive norms).
In terms of programme approaches, no single donor agency working alone can effectively address corruption in the partner country’s health system. It is therefore useful to promote a division of labour among the different development partners based on their respective comparative advantages, experiences, and willingness to engage. It is also useful for health partners to plan ahead and decide who would do what if a corruption incident were to occur in the health sector.
And finally, with regard to coordination among development partners engaged in the health sector: it would be useful to consider contracting a specific anti-corruption, transparency, integrity, and accountability expert with good knowledge of the health sector to work intermittently with the donor group. Such a contractor could help, in particular, with programme coordination with a view to systematically integrating a context-specific anti-corruption and pro-transparency and integrity perspective into health sector initiatives and programmes.
Annex 1. Principal corruption risks and selected mitigation strategies
In order to address corruption in the health sector effectively, it is crucial to identify and understand the problem within each context and to design appropriate counter-measures. Selected strategies based on international experience are described below.
Service user level: Informal payments
Informal payments are charges for health services or supplies meant to be provided free of charge, or payments made informally to public health care providers to obtain specific favours or even basic services. Types of informal payments include, among others, fees paid for treatment, drugs, or expedited/extra services, or offered as an incentive to physicians, nurses, and other health workers to provide better care in the future. It is often difficult to disentangle the specific types of informal payments and to establish whether or not a given payment constitutes corruption. A payment may fall somewhere along a continuum of gravity ranging from gift to bribe to extortion, and from mere nuisance to a serious obstacle to obtaining health care.
Informal payments are sometimes defended as a coping strategy that health workers must use to deal with low pay. However, the frequency of informal payments in the health sector offers an important indicator of underlying governance failures because it means fraudulent behaviour is being tolerated, controls are weak and ineffective, patients are not sure of their rights, and accountability is not enforced. Informal payments tend to be more widespread in settings where the probability of being detected and penalised is very low, as is the case in many developing and transition countries.
Mitigation strategies
The design of mitigation strategies needs to take into account intentions. Are informal payments seen as voluntary contributions by patients to cover the cost of service, or are they an abuse of power by the provider? Depending on the cause of the problem, there are several strategies that can be selected or used in combination.
Formalise user fees
Informal payments can be replaced by formal fee schedule. Payments should be transparent and monitored, and the money should stay in the health sector, with decentralised retention of revenue to supplement salaries, purchase essential supplies, and increase quality of care. This may lead to greater patient satisfaction and encourage overall use of services. However, the introduction of formal fees can also create barriers to equitable access, and such policies therefore require exemptions or subsidies to accommodate the poor. These are best accomplished through a sliding scale, and most countries have adopted some form of means test for patients.
Increase provider/health worker remuneration
Since informal payments may constitute a significant share of income for some health workers, the removal of informal payments may need to be compensated by higher salaries. Linking bonuses to performance can also motivate staff to provide better care.
Increase transparency and accountability
Clear policies, clear information to patients, and channels for complaints can help reduce informal payments. This includes making patients aware of the official fee schedule and telling patients about mechanisms they can use to ask questions or report concerns. When a formal fees are introduced, oversight by facility governance structures such as hospital boards, by external fiduciaries, and by citizens can increase accountability and deter abuse. (Strategies to prevent theft of formal user fees are discussed below.)
Health provider level: Procurement and fraud
Hospital-based expenditures and procurement of drugs, equipment, and supplies account for a large share of public health expenditures. Drug procurement can account for as much as 40%–60% of hospital expenditure in low-income countries, whereas in high-income countries it amounts to 5%–10%. Not surprisingly, drug procurement in hospitals is susceptible to a wide range of scams and kickbacks, as well as delivery of substandard or expired products. With respect to equipment procurement, vulnerabilities to corruption increase as the complexity of equipment increases. Asymmetry of information is especially high when technologies are new.
A major type of corruption in hospitals involves collusion between public officials and suppliers. Accountants and purchasing clerks may collude with suppliers to make a deliberate overpayment for an order. The amount of the overpayment is then refunded by the supplier company to the account of the public official as a kickback. The contracting of venues for training or other services that are later cancelled is another avenue for corruption. The amount paid for the venue is transferred back to the account of the public official(s), while the supplier company may withhold a share as its ‘commission’. This type of corruption is encouraged by lack of sanctions and the low probability of getting caught.
Formal user fees are also susceptible to systematic fraud and theft. Personnel may pocket the fees without recording the transaction; use a ‘refund’ account through which the user fee is refunded to a fictitious patient while the money is transferred to the public official’s bank account; or alter receipts after the service is rendered and paid.
Mitigation strategies
Lack of enforced rules, procedures, and accountability allows irregularities in purchasing practices. Accordingly, improvements in administrative and financial procedures can help deter employees from attempting these types of fraud. These procedures are generally part of an organisation’s internal control system. In addition, specific attention should be paid to procurement procedures and controls. Health advisors should consult experts in financial control and procurement to review gaps and design specific interventions. Investments in fraud control need to be considered in decision making, planning, and budgeting, bearing in mind that relatively small investments in technology can often generate great benefits.
Strengthen internal control systems
It is often crucial to increase organisational and human resource capacity in internal and external audit services. This could require investments in additional staff to provide these services, the purchase of equipment such as electronic cash registers, or the introduction of new management procedures such as spreadsheet analysis of variations over time in utilisation and user fee income. The segregation of duties, in particular with respect to financial management and procurement, can help control fraud.
Leverage procurement and information technology (IT)
The use of IT tools, including procurement databases, to regularly monitor prices of common goods can increase transparency. Procurement fraud can be discouraged by holding purchasing managers accountable if the prices paid differ substantially from benchmark prices or from prices paid by other hospitals. It is important to complement moral suasion with tangible sanctions. The use of fraud detection software is useful and helps reveal patterns of corruption and collusion.
Increase transparency and accountability
In addition to audits and information technology, fraud detection requires mechanisms that beneficiaries and employees can use to raise concerns without fear of retaliation. Complaint boxes, hotlines, and other such mechanisms can be provided.
Strengthen competencies for equipment procurement
Equipment audits as well as the inclusion and monitoring of annual maintenance contracts are useful tools.
Health provider level: Absenteeism
Absenteeism is a chronic although often unmeasured problem in health systems, especially in developing and transition countries. It can be defined as unauthorised absences by workers during contracted hours. Some reasons for absence may be legitimate: for example, rural health workers may need to travel to larger towns to receive their paycheck, or to fetch supplies and drugs. However, many health workers are absent without authorisation and receive wages without providing even minimal services. Civil servants who have high job security, who are subject to minimal supervision, and/or who feel underpaid or overworked may be most susceptible to bending the rules.
Mitigation strategies
Many performance problems, including absenteeism, stem from weak governance systems that fail to reward good performance and to discipline workers who underperform. Strategies to counter the problem emphasise incentives, supervision, and sanctions.
Offer effective incentives
Financial incentives matter but are not the sole solution. A first step is to conduct an assessment of whether health sector wages are actually low relative to comparable private sector wages, as this may not always be the case. If warranted, financial incentives should be accompanied by accountability mechanisms, as financial incentives in an environment of impunity will not be as effective as hoped. They can also be combined with nonfinancial incentives such as career development opportunities, a good work environment, and availability of resources and equipment. Housing and transport may also be important motivating factors.
Implement frequent inspections and peer supervision
Unannounced site visits and community monitoring of health worker presence at the facility level may help reduce absenteeism. However, it is important to design measures that are appropriate in a given cultural context and to ensure regular close monitoring of effectiveness and potential undesired results.
Impose sanctions against workers who are absent without authorisation
Increasing the perceived probability of detection and penalties can lower absenteeism. Sanctions can include reduction in salary, dismissal, transfer to another location, and public shaming by publicising attendance lists at facility level.
Hire contract health workers
Civil servants who have permanent contracts and thus enjoy job security may have higher absentee rates than contracted health workers who can be terminated. This highlights the importance of accountability for reducing absenteeism and raising performance. Local control (e.g., by health or hospital boards or communities) and renewable contracts may reduce absenteeism and improve health services.
Provide information to communities
Simply informing community members of their rights to health care services and of the level of service that the government has contracted (e.g., the number and schedule of office hours per week) can have a significant impact on actual utilisation of services, with a corresponding improvement of health care outcomes. This may need to be combined with an effective complaints-handling mechanism to ensure that providers who fail to show up for work are held accountable.
Health payer level: Financial management (embezzlement, fraud, procurement irregularities)
Without funding, public health care services grind to a halt. Resources for health, once allocated, flow through various layers of national and local government institutions on their way to health facilities. Political and bureaucratic leakage, fraud, abuse, and corrupt practices can occur at every stage of the process. Contributing factors include poorly managed expenditure systems, lack of effective auditing and supervision, organisational deficiencies, and lax fiscal controls over the flow of public funds (Table A.1).
Before funding even begins to flow, there are risks for abuse in decision making about how funds will be allocated and spent. Health personnel may be told there is ‘no money in the budget’ for a specific need when in fact the money is there, but a corrupt officer wants to divert it to a pet project or favourite staff member’s department instead of the intended use. Medical staff often assume that worrying about finance is not their job, but this leaves decision making vulnerable to abuse by administrative staff who may not understand the goals of the health sector.
Budget leakages, meaning the discrepancy between the authorised budget for health and the amount of funds received by intended recipients, may occur at multiple points in the health system. For example, funds at central level may be diverted before they reach the provincial level; funds that reach the province may be embezzled by provincial-level staff; or a cascade of outflows can create leakages across multiple levels. Budget leakages can take different forms, including the diversion of public funds into private accounts, mismanagement and corruption in procurement, and payroll irregularities associated with ghost workers (personnel who are listed on payroll but who no longer, or never did, work for the ministry of health or a lower level of government).
Countries with weak institutions and endemic levels of corruption face serious challenges in the procurement of medical supplies, drugs, equipment, and facility construction (problems in the drug supply chain are discussed below). The absence of a clearly regulated procurement process, incentives for performance, accountability, adequate monitoring and oversight, and controls can lead to last-minute changes to contract provisions, the alteration of contract specifications skewed towards a certain bidder, and the influencing of negotiations through kickbacks.
Table A.1: Overview of vulnerabilities in public financial management relevant to health
| Area of public financial management | Vulnerabilities |
| Budget planning and execution |
|
| Employee compensation |
|
| Goods and services |
|
| Transfers |
|
| Capital expenditures |
|
Source: Adapted from Lewis and Pettersson (2009).
An added complication is that the health sector sometimes has sizeable off-budget accounts. Donor funds are the most important external resource in many developing countries, particularly in Africa. Despite the trend towards pooled funding, a considerable share of donor funds continues to be channelled off-budget through international and non-governmental organisations.edab2c7b5043 There is an inherent risk of corruption when large amounts of funding become available and need to be spent quickly, as has been the case with some HIV/AIDS-related funding in developing countries under the Global Fund and PEPFAR initiatives. Often these funds are placed outside the review of regular budget allocation, discipline, and oversight processes.
Mitigation strategies
Addressing corruption risks in the financial management system of the health sector requires a combination of measures and collaboration with institutions across government, including first and foremost the ministry of finance (MOF).e86cebd94be6 Public financial management reforms are often led by MOF staff, but health personnel must also own these reforms to ensure they are fully implemented in the health sector. This may require changes in how health leaders see their own jobs: not only as medical personnel focused on health interventions, but also as managers and stewards of resources.
Use Public Expenditure and Financial Accountability (PEFA) indicators
These indicators can be used to identify points in the budget process where governance problems exist. For example, a low score on one crucial indicator – availability of information on resources received by service delivery units – suggests some combination of inadequate transparency, poor record keeping, low budget management capacity, and insufficient accountability. PEFA indicators can be helpful in pinpointing and prioritising areas where action is needed to strengthen budget processes and help bolster good governance in public financial management (Table A.2).
Table A.2: PEFA indicators relevant to health
| Predictability and control in budget execution | Budget credibility | Budget comprehensiveness and transparency |
|
|
|
| Policy-based budgeting | Accounting, recording, and reporting | External scrutiny and audit |
|
|
|
Source: Lewis and Pettersson (2009).
Track resource flows
Measuring resource leakages and efficacy of public spending is an important means to detect problems. Public Expenditure Tracking Surveys (PETS), Public Expenditure Reviews (PER), Quantitative Service Delivery Surveys, and price comparisons can identify places where funds are not reaching beneficiaries or are being used for non- intended purposes. They complement PEFA evidence about government-wide performance, offering an important diagnostic on budget management and leakages. It is critical to pair this kind of diagnostic with other interventions that build demand for reforms in budget management, putting pressure on public systems to improve.
Improve budgeting and accounting systems
Health systems require a legal and institutional framework that provides clear accounting and procurement standards based on transparency, comprehensiveness, and timeliness. They should have effective reporting, supervision, and auditing systems to improve fiscal oversight and ensure effective enforcement of rules and sanctions for financial misconduct. Even so, there may be resistance from those who stand to benefit from corruption in the system.
Increase internal transparency
The aim is to ensure that information and data are recorded accurately and on a regular basis, that information is available to decision makers on demand, and that decision makers feel confident in their ability to read and analyse reports. This requires better information management systems (with respect to accuracy, timeliness, and distribution of financial information); training of staff in their application and use; sensitisation of stakeholders in how to use information for accountability; and, crucially, the introduction of expectations and incentives for regular data collection, maintenance, and use.
Strengthen external audits
Audits can detect financial irregularities and suggest ways to rectify problems. To minimise the time and cost of audits, health and finance ministries can simplify their records and streamline procedures. Local capacity for audit in many countries is extremely limited. Capacity strengthening for private sector firms, even firms affiliated with international accounting agencies, is needed. Additionally, health advisors need to develop clear terms of reference for performance audits, which can detect fraud by verifying that suppliers exist, purchased equipment is working, and so on. Too often, audits are designed to verify only that rules are followed, and auditors do not have the special skills required to detect problems such as ghost suppliers, faked invoices, or collusion.
Use e-procurement to improve efficiency and discourage corruption
Electronic government procurement can increase transparency and accountability in health procurement, thereby improving resource management, reducing opportunities for fraud, and, ultimately, leading to lower prices. Procurement databases are useful for price comparisons. The introduction of fraud detection software helps identify collusion or red flags that normal audits may fail to spot.
Promote budget transparency and participation
Civil society must be enabled to take part in the budget process, both in formulating budgets and in monitoring their use. Participatory budgeting initiatives encourage a wide range of stakeholders to play a role in allocating budgets according to their community’s priorities, in monitoring budgets to ensure that spending is in accordance with those priorities, and in monitoring the quality of goods and services purchased with budgets. The government’s capacity to function as auditor and supervisor in weak institutional environments is very limited. Involving community organisations, professional associations, and other non-governmental bodies through dissemination of information will help monitor and challenge abuses and combat the culture of impunity.
Health payer level: Personnel management (ghost workers, purchase of positions and promotions)
The public sector health workforce represents the largest single group of civil servants in most countries, and as a result, the health sector claims a significant proportion of national budgets. When health workers are hired and paid at central level (by the ministry of health) but are assigned to health facilities locally, their lines of reporting and accountability become opaque, as does managerial authority. In addition, management information on even simple things such as attendance is often lacking. In a situation marked by minimal information, conflicting incentives, and weak accountability, there are risks of abuse and corruption.
One serious problem is payroll irregularities, in particular the existence of ghost workers. The main underlying cause is often a weak personnel information system that fails to accurately record and regularly update the deployment of health staff. However, when ghost workers are on payroll, the culprits are rarely health workers alone – indeed, they may not be involved at all. Rather, administrative staff in charge of maintaining payroll records often have greater opportunity to manipulate records in order to siphon off wage payments.
The processes for hiring and promotion of health workers and health sector administrative staff constitute another area of risk. Bribes can play a key part in the selection process. In some countries, positions for physicians and others can be ‘bought’ from health facility committees, board members, or ministerial staff. As a consequence, the recruitment and selection of health workers and administrators may be influenced by candidates’ ability and willingness to pay for positions rather than by objective criteria. At the service delivery level, this may lead newly hired health workers to demand fees from patients in order to recover their own ‘investment’ in the position. Similarly, administrators may engage in fraud or embezzlement to recoup their initial payment.
Mitigation strategies
Clean up and manage payrolls
Regular updating of employee lists and payroll commitments is a basic management tool and a high priority for health systems, which have large numbers of employees. Physical verification at points of payment can be carried out. A less costly method is to have auditors conduct spot checks at health facilities to verify that workers on payroll actually exist and are on the job.
Ensure transparent recruitment, assignment, and promotion systems
Procedures based on clear rules and criteria known to all relevant parties tend to reduce the scope for fraudulent practices. Hiring and promotion by selection committees is preferable to actions by a single administrator since it limits discretion and improves credibility if the procedures are transparent. Moldova implemented such a system in 2007, requiring all existing directors of facilities to reapply for their jobs. It should be noted, however, that promoting transparency and merit in recruitment, assignment, and promotions is often politically and administratively difficult. In some countries the hiring and promotion of health staff may be part of a corrupt patronage system that is more difficult to break than individual abuses.
Use the private sector to speed up recruitment and deployment
Where public recruitment systems function poorly, the private sector for recruitment can sometimes provide a faster and more effective alternative. Under the supervision of the relevant public sector institutions (ministries of health, finance, and others), a private company may be hired to recruit, deploy, pay, and manage, through an agreed fast-track hiring system, the contracts of newly recruited health workers, who are later transferred to government payroll.
Health payer level: Drug supply, procurement, and distribution
In order to ensure drug safety and an efficient allocation of resources, the very lucrative pharmaceutical sector is under government regulation throughout the life cycle of medical products. Although this regulation should improve efficiency, it also provides openings for corruption at every stage of the regulatory process: during drug manufacturing, registration (of medicines and pharmacies), selection, procurement, distribution, prescription, and dispensing (Table A.3). Drugs move through a supply chain that is extremely complex – sometimes including more than 30 parties – before reaching end users.
Table A.3: Corruption in the drug supply (value) chain: Key risks and counter-strategies
| Decision point | Processes | Strategies |
| Manufacturing |
|
|
| Registration |
|
|
| Selection |
|
|
| Procurement |
|
|
| Distribution |
|
|
| Prescribing and dispensing |
|
|
Source: Adapted from Cohen , Mrazek, and Hawkins (2007).
Mitigation strategies
Reducing discretion and increasing transparency and accountability are particularly relevant in the pharmaceutical sector. Otherwise, regulators can easily be captured, and the decision points and processes of the drug supply chain will be open to corrupt schemes by individuals or groups. A systems approach is needed. The following strategies are particularly relevant for mitigating risk in the drug supply chain.
Engage the WHO Good Governance for Medicines (GGM) programme
GGM helps foster transparency and create clear administrative procedures for the procurement of drugs. In addition, the programme promotes the ethical conduct of health workers.
Establish or strengthen an independent drug regulation agency
As recommended by WHO, this needs to be accompanied by strong laws and regulations that ensure transparency as well as uniform and effective application of the defined standards. Many drug regulatory agencies are understaffed and lack technology. Others could use help in leadership development, strategic planning, and management systems. Where financial resources are limited and a full drug laboratory, for example, is not available, reliance on drugs that have gone through the WHO prequalification process could be considered.
Strengthen drug management systems
Investments in greater security and control in the warehousing and distribution of drugs can prevent theft. Commercial best practice shows that there are logistics management techniques that can safeguard stock. This type of approach is often funded as a health systems strengthening activity, but it has obvious benefits for controlling corruption as well.
Leverage information technology
Use of information technology can increase transparency and accountability. This may include establishment of online drug price catalogues; publication of tenders, adjudication decisions, and monitoring results on the internet; and use of e-procurement tools for drugs and medical supplies. The persons who disclose information need to be committed and trained, the accuracy of information needs to be ensured, and the recipients of the information need to be empowered to use the information for monitoring and advocacy purposes.
Enforce transparency and accountability in decision-making processes
This means opening up the different decision-making processes to participation of stakeholders; ensuring active disclosure of information to interested parties; and holding the actors involved accountable for their decisions and results, including through public naming and shaming.
Promote self-regulation of the pharmaceutical industry and professional associations
The pharmaceutical industry has an interest in avoiding reputational risks, in particular by preventing infiltration of counterfeit drugs. And while members of health professions enjoy extensive discretionary power, these professions also recognise and enshrine high ethical standards. Efforts should be made to promote adherence to and effective enforcement of codes of conduct of the pharmaceutical industry (e.g., International Federation of Pharmaceutical Manufacturers Associations) as well as of medical professional associations (e.g., through the World Medical Association’s International Code of Medical Ethics).
- 2011.
- Hanf et al. (2011).
- Collignon et al. (2015).
- Friedman (2018).
- Bruckner (2019), p. 7. This report, published by the Transparency International Health Initiative, provides an excellent overview of the description, drivers, prevalence, and impact of corruption in health at the service delivery level.
- 2013 Transparency International Global Corruption Barometer, cited in Bruckner (2019), p. 9.
- Bate (2011), cited in Bruckner (2019), p. 11. Unless otherwise indicated, all monetary amounts in this Issue are US dollars.
- National Academies of Sciences, Engineering, and Medicine (2018).
- Cited in Bruckner (2019), p. 12.
- See, e.g., Ozawa et al. (2018).
- See, e.g., Vian, Savedoff, and Mathisen (2010); Lewis and Pettersson (2009); U4 (2008).
- Bruckner (2019), p. 2.
- Sommersguter-Reichmann, Wild, and Stepan, et al. (2018).
- Delavallade (2006).
- Vian et al. (2011).
- Bruckner (2019), pp. 2–3.
- See the WHO web page on UHC.
- Jones and Jing (2011) and WHO (2018c), cited in Bruckner (2019), p. 2.
- WHO (2018c).
- Data from OECD.Stat.
- In a slight variation, Norad (2008) defines corruption as ‘the abuse of entrusted authority for illicit gain.’
- Those in the private sector who willingly collaborate with corrupt government officials are equally guilty of corrupt practices when they offer and/or pay bribes in order to obtain an advantage for their firm. The same goes for employees of civil society or international organisations who embezzle funds or resort to bribes to win certain public contracts.
- For more information, see Savedoff and Hussmann (2006); Hussmann (2011b).
- In many developing countries, faith-based organisations provide health services in partnership with government and form the backbone of the rural health system. This mix of public and private providers complicates budget transparency and the definition of accountability relationships. Faith-based organisations are not free from corruption risks.
- See Bruckner (2019) for an overview of these practices and an annotated bibliography.
- Complaints mechanisms may be located within the health facility or the ministry of health. They may also be run by a national anti-corruption commission or by a legal assistance centre such as Transparency International’s Advocacy and Legal Advice Centres (ALACs), now operating in more than 60 countries.
- Political commitment is difficult to assess. There is a tendency to overestimate the commitment of senior public officials to reform and to underestimate political challenges they will face in delivering on promises if they are serious.
- National Academies of Sciences, Engineering, and Medicine (2018).
- Gaitonde et al. (2016).
- OGP (2019).
- Resolution 72.8, adopted by the 72nd World Health Assembly in May 2019.
- Transparency International UK (2017).
- Schaaf (2018). Social accountability refers to actions by citizen groups to hold public officials and service providers accountable for their performance in delivering services and protecting people’s rights.
- Björkman and Svensson (2009); Björkman, de Walque, and Svensson (2012). See also Golub (2020).
- Gullo et al. (2017).
- This section draws on and quotes from a WHO online fact sheet on UHC.
- WHO adds that ‘protecting people from the financial consequences of paying for health services out of their own pockets reduces the risk that people will be pushed into poverty because unexpected illness requires them to use up their life savings, sell assets, or borrow.’
- Mackey, Vian, and Kohler (2018).
- Gaitonde et al. (2016).
- Examples of initiatives in other sectors include the Extractive Industries Transparency Initiative (EITI) and the Infrastructure Transparency Initiative (CoST), among others.
- Examples include the Global Fund to Fight AIDS, Tuberculosis and Malaria; Gavi, the Vaccine Alliance; and the Health Results Innovation Trust Fund (HRITF).
- Disch and Natvig (2019); Taylor and Harper (2014).
- See García (2019).
- For valuable inputs and illustrations, see Mackey, Vian, and Kohler (2018).
- The second OGP Action Plan for Colombia, for example, included commitments from the health sector aimed at addressing opacity and corruption risks in the pharma sector (especially in the areas of drug prices, prescription patterns, and relations between the industry and health professionals).
- Existing initiatives include, among others, the DFID-funded Anti-Corruption Evidence Programme, which looks at corruption in the health sector among others; the University of Toronto’s WHO Collaborating Centre for Governance, Accountability, and Transparency in the Pharmaceutical Sector; and the Boston University–based Act for Health programme, which promotes accountability and transparency for health through research, consulting, and teaching.
- Language may be critical in achieving official buy-in. Where possible, indicators on corruption should be framed as such, but in more sensitive contexts it may help to use neutral terminology, such as ‘development effectiveness’. However, such abstract language risks losing sight of the problem.
- In Colombia, the regional EUROsociAL II programme provided support for peer-to-peer initiatives to improve transparency and access to information on drug-related issues, while the bilateral ACTUE Colombia project worked to foster transparency and integrity in a variety of sectors. These approaches together helped consolidate the initiatives around transparency of drug prices, use, and prescription.
- In high-level political dialogue in particular, focusing on ‘corruption’ as such may be too sensitive, and a positive goal like improving ‘value for money’ or ‘development effectiveness’ may be more desirable. However, at a technical level it is important to build an evidence base on vulnerabilities to and actual levels of corruption.
- An OECD DAC (2010) document on working towards more effective collective donor responses to corruption offers the following guidance: (a) prepare collectively in advance for responses; (b) follow the government lead where this exists; otherwise foster this lead, promote accountability, and coordinate donors; (c) agree in advance on a graduated response if performance stagnates or deteriorates; (d) act predictably in relation to other donors; encourage other donors to respond collectively to the extent possible, but allow flexibility for individual donors; (e) maintain dialogue at different levels and focus on long-term development objectives; (f) foster accountability and transparency in country and internationally; (g) act internationally but link international action to anti-corruption work in partner countries.
- In the United States, the Physician Payments Sunshine Act requires drug and medical device companies to disclose the payments they make to doctors. A number of other countries have similar laws.
- U4 has published broadly on health topics.
- For example, the Global Fund has committed 50% of its resources directly to governments and an almost equally large share to other organisations and the private sector.
- Regrettably, one cannot assume that the finance ministry itself is free of corrupt practices. It is not uncommon, for example, for MOF staff to require unauthorised payments in exchange for the release of budgeted funds. Health advisors should discuss these issues with their colleagues and with their peers on governance teams.